Pancreas
Pancreas . Ali B Alhailiy. pancreas. The pancreas is a glandular organ in the digestive systemand endocrine system.

Pancreas
E N D
Presentation Transcript
Pancreas Ali B Alhailiy
pancreas • The pancreas is a glandular organ in the digestive systemand endocrine system. • It is an endocrine gland producing several important hormones, including insulin, glucagon, somatostatin, and pancreatic polypeptide which circulate in the blood. The pancreas is also a digestive organ, secreting pancreatic juice containing digestive enzymes that assist digestion and absorption of nutrients in the small intestine. These enzymes help to further break down the carbohydrates, proteins, and lipids .
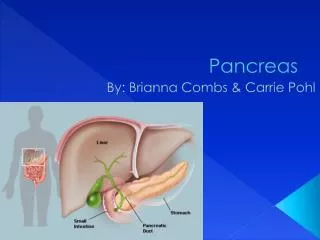
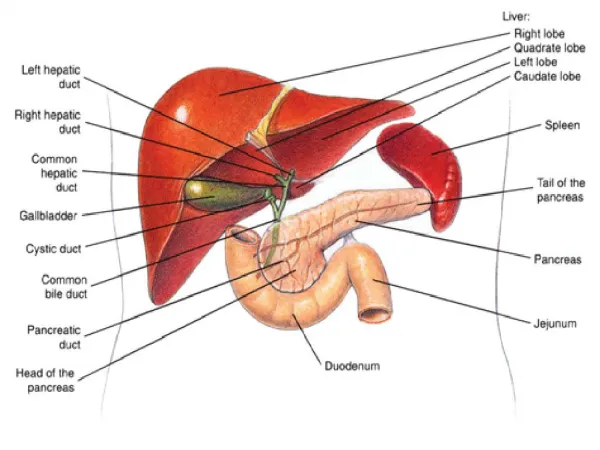
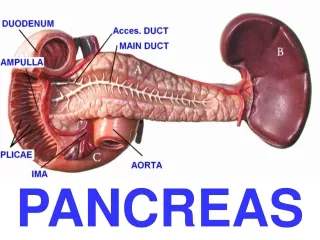
Structure • The pancreas is an endocrine organ that lies in the abdomen, specifically the upper, left abdomen. It is found behind the stomach, with the head of the pancreas surrounded by the duodenum. The pancreas is typically 5.75-9.5 cm long.
Structure • Anatomically, the pancreas is divided into a head, which rests within the concavity of the duodenum, • a body lying behind the base of the stomach, • and a tail, which ends abutting the spleen. • The neck of the pancreas lies between the body and head, and is in front of the superior mesenteric artery and vein. • has two main ducts, the main pancreatic duct, and the accesory pancreatic duct. These drain enzymes through the Ampulla of Vater into the duodenum.
Function B - Exocrine • The pancreas as an exocrine gland helps out the digestive system. It secretes pancreatic fluid that contains digestive enzymes that pass to the small intestine. These enzymes help to further break down the carbohydrates, proteins and lipids (fats) . • In humans, the secretory activity of the pancreas is regulated directly via the effect of hormones in the blood on the islets of Langerhans. • The exocrine component of the pancreas, often called simply the exocrine pancreas, is the portion of the pancreas that performs exocrine functions. It has ducts that are arranged in clusters called acini(singular acinus). Pancreatic secretions are secreted into the lumen of the acinus, and then accumulate in intralobular ducts that drain to the main pancreatic duct, which drains directly into the duodenum. • Control of the exocrine function of the pancreas is via the hormones gastrin, cholecystokinin and secretin, which are hormones secreted by cells in the stomach and duodenum, in response to distension and/or food and which cause secretion of pancreatic juices
Function • The pancreas is a dual-function gland, having features of both endocrine and exocrine glands. A- Endocrine • The part of the pancreas with endocrine function is made up of approximately a million cell clusters. Four main cell types exist in the islets .they can be classified by their secretion: • α (alpha) cells secrete glucagon (increase glucose in blood), β (beta) cells secrete insulin (decrease glucose in blood), Δ (delta) cells secrete somatostatin (regulates/stops α and β cells) and PP cells, or gamma cells, secrete pancreatic polypeptide. • The islets of Langerhans play an imperative role in glucose metabolism and regulation of blood glucose concentration.
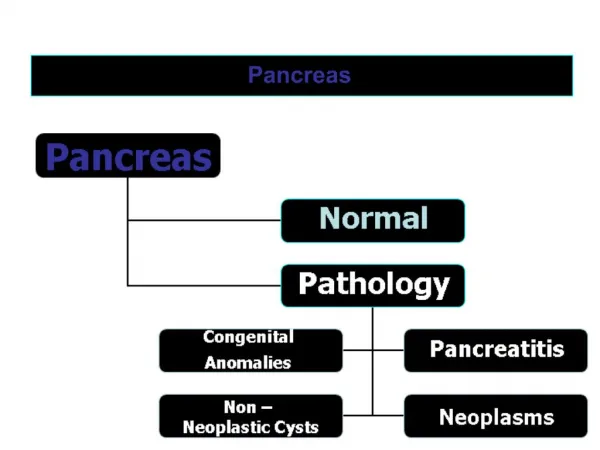
PATHOLOGY • 1- Pancreatitis • Pancreatitis is inflammation of the pancreas. There are two forms of pancreatitis, which are different in causes and symptoms, and require different treatment: • Acute pancreatitis is a rapid-onset inflammation of the pancreas, most frequently caused by alcoholism or gallstones. • Chronic pancreatitis is a long-standing inflammation of the pancreas. • 2- Diabetes mellitus • The pancreas is central in the pathophysiology of both major types of diabetes mellitus. In type 1 diabetes mellitus, there is direct damage to the endocrine pancreas that results in insufficient insulin synthesis and secretion. Type 2 diabetes mellitus , which begins with insulin resistance , is characterized by the ultimate failure of pancreatic β cells to match insulin production with insulin demand.
3- Exocrine pancreatic insufficiency • (EPI) is the inability to properly digest food due to a lack of digestive enzymes made by the pancreas. EPI is found in humans afflicted with cystic fibrosis. It is caused by a progressive loss of the pancreatic cells that make digestive enzymes. Chronic pancreatitis is the most common cause of EPI in humans.. • 4- Cystic fibrosis • Cystic fibrosis, is a hereditary disease that affects the entire body, causing progressive disability and early death. It is caused by a mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. The product of this gene helps create sweat, digestive juices, and mucus. The name cystic fibrosis refers to the characteristic 'fibrosis' (tissue scarring) and cyst formation within the pancreas, causing irreversible damage, and often resulting in painful inflammation (pancreatitis).
5- Cysts • (CT scan) findings of cysts in the pancreas are common, and often are benign. • In a study of 2,832 patients without pancreatic disease, 73 patients (2.6%) had cysts in the pancreas.About85% of these patients had a single cyst. Cysts ranged in size from 2 to 38 mm (mean, 8.9 mm). There was a strong correlation between the presence of cysts and age.
6- pancreatic mass • A pancreatic mass is any undifferentiated growth detected in the pancreas, usually on medical imaging. • Masses can be described based on their physical characteristics, as defined by imaging studies, as solid (consisting of solid abnormal tissue) or cystic (cavitie filled with mucus or fluid such as pseudocysts,” . • correct diagnosis.
Signs and symptoms • A-The clinical history can often help establish the nature of a tumor involving the pancreas. For example, a history of alcoholismcomplicated by multiple episodes of pancreatitissuggests the possibility of a pseudocyst, the leakage and collection of pancreatic enzymes outside of the pancreas. By contrast, patients with painless jaundice(an abnormal yellowing of the skin and eyes often caused by blockage of the bile ducts) are more likely to have a pancreatic cancer. B- Blood testscan also point to the correct diagnosis. Patients with pseudocysts often have associated pancreatitis with elevated blood levels of the enzymes amylase and lipase, while patients with pancreatic cancer may have elevated levels of the cancer marker .
C-medical imaging • A number of different approaches can be used to visualize the pancreas. The most common include CT scan), magnetic resonance imaging (MRI), positron emission tomography (PET), endoscopic ultrasound (EUS), and endoscopic retrograde pancreatography (ERCP). Each of these different imaging approaches has its own strengths and weaknesses. • CT scanning is a widely available and an excellent modality to image the pancreas. • MRI is a great method to visualize the pancreatic ducts, PET scanning can reveal the metabolic activity of a tumor. • ERCP can be used to visualize the duct system of the pancreas and stents (small tubes to re-establish the flow of secretions such as bile) can be placed during the ERCP procedure.
Endoscopic retrograde cholangiopancreatography (ERCP) • Endoscopic retrograde cholangiopancreatography (ERCP) is a technique that combines the use of endoscopy and fluoroscopy to diagnose and treat certain problems of the biliary or pancreatic ductalsystems. • Through the endoscope, the physician can see the inside of the stomach and duodenum, and inject radiographic contrast into the ducts in the biliary tree and pancreas so they can be seen on X-rays. • ERCP is used primarily to diagnose and treat conditions of the bile ducts and main pancreatic duct, including gallstones, inflammatory strictures (scars), leaks (from trauma and surgery), and cancer.
. ERCP can be performed for diagnostic and therapeutic reasons. • The development of safer and relatively non-invasive investigations such as magnetic resonance cholangiopancreatographY (MRCP) and endoscopic ultrasound has meant that ERCP is now rarely performed without therapeutic intent.
Magnetic resonance cholangiopancreatography (MRCP) • (MRCP) is a relatively new MR imaging technique that is used for noninvasive work-up of patients with pancreaticobiliary disease. • Recent studies have shown that MRCP is comparable with invasive (ERCP) for diagnosis of extrahepatic bile duct and pancreatic duct abnormalities such malignant obstruction of the bile and pancreatic ducts, congenital anomalies ,and chronic pancreatitis . In some institutions, MRCP is becoming the initial imaging tool for the biliarysystem.
Technique • By using T2-weighted sequences, the signal of static or slow-moving fluid-filled structures such as the bile and pancreatic ducts is greatly increased. • The coronal plane is used to provide a cholangiographic display. • the axial plane is used to evaluate the pancreatic duct and distal common bile duct. • In addition, some institutions perform three-dimensional reconstruction by using a maximum-intensity projection (MIP) algorithm on the thin-collimation source images increased duct-to-background contrast.
advantages of MRCP • indication for ERCP are unsuccessful ERCP and contraindication to ERCP . • Although ERCP is still the standard of reference for imaging the pancreatico-biliary system • there are specific advantages of MRCP over ERCP. MRCP (a) is noninvasive; (b) is cheaper; (c) uses no radiation; (d) requires no anesthesia; (e) is less operator dependent; (f) allows better visualization of ducts proximal to an obstruction; and (g) when combined with conventional T1- and T2-weighted sequences, allows detection of extraductal disease.
Disadvantages of MRCP • include (a) decreased spatial resolution, making MRCP less sensitive to abnormalities of the peripheral intrahepatic ducts (eg, sclerosingcholangitis) and pancreatic ductal side branches (eg, chronic pancreatitis); and (b) imaging in the physiologic, nondistended state, which decreases the sensitivity to subtle ductal abnormalities. Furthermore, the main criticism of MRCP is that appropriate care is delayed in patients who need therapeutic endoscopic or percutaneous intervention of obstructing bile duct lesions.
Thus, it is argued that in patients with high clinical suspicion for bile duct obstruction, ERCP should be the initial imaging modality to provide timely intervention (eg, dilatation, stent placement, stone removal) if necessary.
A small enhanced mass (arrow) in the pancreatic tail is demonstrated at the arterial phase of -MRI
Abdominal MRI coronal view of heterogeneous, well circumscribed mass in the head of the pancreas