Download
1 / 45
450 likes | 752 Vues
Community Dental Health Coordinator (CDHC) An integrated model to reduce disparities in oral health. Agenda. The access to dental care paradox? Frameworks for developing solutions for the access problem Community Dental Health Coordinator Scope of services Education Next steps.

E N D
Community Dental Health Coordinator (CDHC)An integrated model to reduce disparities in oral health
Agenda • The access to dental care paradox? • Frameworks for developing solutions for the access problem • Community Dental Health Coordinator • Scope of services • Education • Next steps
Define the Problem? The way we see the problem, is the problem. Steve Covey
Problem #1 • Not enough dentists • Cannot find dentists to work in underserved areas • Dentists do not accept Medicaid • Dentists are rich and they do not care • Dentists…. • Dentists…
Solution #1 • Train more dentists • or • Provide incentives for dentists to work in underserved areas • or • Train alternatives providers • or • Ask why dentists do not do it?
Solution #1 • These solutions will work if the problem is the “dentist” • However, if the problem is • Organization of dental care • Reimbursement • Cultural, economic, social, behavioral barriers both facing the dentists and underserved populations, then • These solutions will not work
Push pins are private practice dentists. Detroit and Suburbs: 2005 Projected Household Income by Census Tract
Define the problem! • 0.2% out of the 18,000 children <1 year old • 0.8% out of 26,000 children <1 year old
Define the problem! • 15% out of the 168,000 children (2-21 years) • 42% out of 203,000 children (2-21 years)
Problem #2: If we see them they will be fine • Self-care + access • What type of access? • Preventive • Restorative • Disease management is the road to recovery • We will fill our way out of the problem • We will seal our way out of the problem • We will scale our way out of the problem
The Dental and Medical Care Paradox • Whitehall study of civil servants in the UK • Social gradient of disease • Allostatic load • Social support, efficacy, fatalism, literacy • Universal health care • Equality of primary and basic access to healthcare but the inequalities in health outcomes will persist
Access to dental care is not a dental problemAccess is necessary but not sufficient factor in reducing the inequalities in health outcomes
Who is responsible for the problems of dental access and oral health disparities?
Multi-level Responsibility • National and state policy • Medicaid • Community health centers • Tax policy • Welfare policies • Educational standards and funding • Agriculture quota • Research funding • Globalization and free trade
Multi-level Responsibility • Local policy • Crime • Transportation • Education • Taxation • Economic development • Investment in health care • Public health versus tertiary care
Multi-level Responsibility • Individual level • Dental anxiety • Locus of control (fatalism) • Oral heath self-efficacy • Social support • Role models • Education • Employment • General and social health
Multi-level Responsibility • Family level • Family structure • Child care • Employment • Safety net • Social support
Framework or roadmaps or blueprints Frameworks are tools for Defining problems Designing solutions Evaluating outcomes Instructions versus Self-Determination Theory I will tell you what to do versus what would you like to do? What is important to you?
Community Health Workers • Community health workers are trained to promote health in their own communities. They provide leadership, peer education, and resources to support community empowerment. • CHWs integrate information about health and the health care system into the community’s culture, language, and value system, thus reducing many of the barriers to health services Ro et al., 2007
Community Health Workers • CHWs offer interpretation and translation services, provide culturally appropriate health education and information, assist people in receiving the care they need, give informal counseling and guidance on health behaviors, advocate for individual and community health needs, and provide some direct services such as first aid and blood pressure screening
Effectiveness: CHWs • Improved access for minority women in • prenatal care, • cancer screening, • child sick visits, • immunizations for children, • chronic illness care, • maternal health, • STD testing, • smoking cessation, and • mental health and outreach services.
Effectiveness: CHWs • Influenced positive behavioral changes in the areas of weight loss and breastfeeding among African Americans, • Reduced drug use • Increased condom use among homeless women, • Increased physical activity among African-American women with type II diabetes
Effectiveness • Reduced missed appointments and increase follow-up care.
CDHC • Dual skills • CHWs • Dental skills • Extenders of the supervising dentist, the decision maker • Could increase the efficiency and reach of PA 161 hygienists • Dentists is RESPONSIBLE for dental care • No cavitated teeth should be left behind unless it is appropriate • Triage • Care process and team approach • Quantity is key for survival in the underserved zone • Quality should be outcome driven
The CDHC’s Main Functions Recruitment and registration Screening for emergencies Patient navigation Oral health assessment Navigation with dentists and hygienists Prevention of dental & oral diseases Palliative care Navigation with dentists and hygienists Develop tailored preventive plans Recall based on risk status
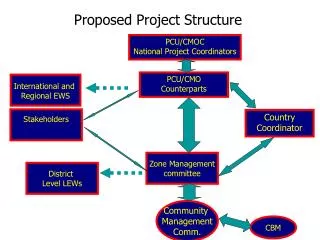
PalliativeCare Community Dental Health Coordinator Integrated Dental Care System Oral Health Promotion Prevention of Dental/ Oral Diseases Improve access to dental care and reduce oral health disparities Patient Navigation
CDHC: Entry Tracks • High school graduates • 1 year didactic + practical training at a CODA accredited program • 6-month internship • Dental assistants • Modules (TBD): < 1 year • 6-month internship • Dental hygienists • Modules (TBD): < 1 year • 6-month internship • Other healthcare and health service providers • Social workers • Nurses
VISION Integrated Dental Care System
Promotora VISION Improve access to dental care and reduce oral health disparities Oral Health Promotion Health promotion is the science & art of helping people change their lifestyle to move toward a state of optimal health
VISION Improve access to dental care and reduce oral health disparities Palliative Care Manual Restorative TreatmentInterim (temporary) restorations
Scaling Perform gross debridement in community settings which may include scaling using anterior and/or posterior sickle hand scalers for patients with Perio type I (gingivitis) and have calculus that impedes maintaining good oral hygiene. Once scheduled, the patient will be seen by the dental hygienist or dentist at the community health centers.
VISION Improve access to dental care and reduce oral health disparities Patient Navigation Entry into and Movement through a Complex Bureaucratic Healthcare System Eligibility for Medicaid and other programs Registration
CDHC Curriculum • Community health worker & health promotion modules • Advocacy and outreach • Communication & cultural competency • General & motivational interviewing skills • Coordination, documentation & reporting • Teaching & learning skills • Legal & ethical issues
CDHC Curriculum • Dental Skills Modules • Introduction to dentistry • Screening & classification • Prevention of dental caries • Prevention of periodontal diseases • Prevention of oral cancer • Palliative care • Payment for dental care • Clinical support system • Community-based internship
Training • The CDHC will be trained in accredited dental schools or community colleges with dental programs.
Pilot or Demonstration Projects • Three sites for three years • Rural • Urban • Indian tribal area
Budget for each site • Training of CDHCs • Stipends • Portable equipment and maintenance • Coordination • Evaluation • Estimated to be around $300,000 per year for 3 years • ADA has invested over $330K to develop the “turn-key” curriculum • ADA has allocated $2 Million for the pilots • Local funding is required
CDHC: Employment • Community settings • Community health clinics • Schools • WIC clinics • Head and Early Head Start centers • Institutions • Medical and other health clinics (e.g. Indian Health Service, FQHCs)
CDHC: Financing Strategy • Breakeven point • About 600 Medicaid recipients per salaried CDHC ($27,000, total cost is $70,000) • For DH working as a CDHC, the breakeven point will be around 900 Medicaid recipients. • Revenue neutral model that is not dependent on operating grants
CHW Legislation • In the State of Minnesota, CHW Legislation of 2007 was passed. • Covers the care coordination and patient education services provided by a community health worker if the community health worker has: • Received a certificate from the Minnesota State Colleges andUniversities System approved community health worker curriculum; or • At least five years of supervised experience with an enrolledphysician, registered nurse, or advanced practice registered nurse.Community health workers eligible for payment under clause • Must complete the certification program by January 1, 2010, to continue to be eligible for payment • Community health workers must work under the supervision of a … physician, registered nurse, or advanced practice registered nurse.
Integrated Oral Health Promotion and Dental Care Model Ultimately education [health promotion] and prevention will be the linchpins in eliminating… untreated dental disease. ADA’s State and Community Models for Improving Access to Dental Care for the Underserved—A White Paper