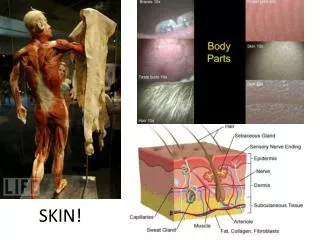
SKIN
SKIN. Surface epithelia are traditionally classified according to three morphological characteristics: The number of cell layers: a single layer of epithelial cells is called simple epithelium , whereas epithelium composed of several layers is a stratified epithelium .

SKIN
E N D
Presentation Transcript
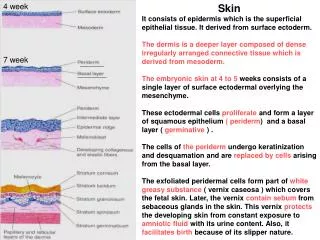
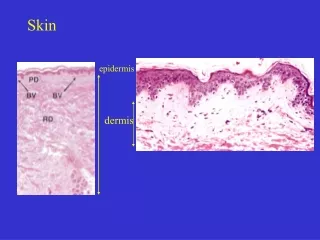
Surface epithelia are traditionally classified according to three morphological characteristics: • The number of cell layers: a single layer of epithelial cells is called simple epithelium, whereas epithelium composed of several layers is a stratified epithelium. • The shape of the component cells: this is based on the appearance in sections taken at right angles to the epithelial surface; cells are thus either squamous (flattened), cuboidal or columnar. In stratified epithelia the shape of the outermost layer of cells determines the descriptive classification. • The presence of surface specialisations such as cilia and keratin. For example the epithelial surface of the skin is classified as stratified squamouskeratinising epithelium since it consists of many layers of cells, the surface cells of which are flattened (squamous) in shape, and it is covered by an outer layer of the proteinaceous material, keratin that is synthesised by the epithelial cells.
Vesicle: Fluid-filled raised lesion 5 mm or less across. • Bulla: Fluid-filled raised lesion greater than 5 mm across. • Blister: Common term used for vesicle or bulla. • Pustule: Discrete, pus-filled, raised lesion. • Wheal:itchy, transient, elevated lesion with variable blanching and erythema formed as the result of dermal edema.
Acantholysis:Loss of intercellular connections resulting in loss of cohesion between keratinocytes • Spongiosis: Intercellular edema of the epidermis • Hydropic swelling (ballooning): Intracellular edema of keratinocytes, often seen in viral infections • Exocytosis: Infiltration of the epidermis by inflammatory or circulating blood cells • Erosion: Discontinuity of the skin exhibiting incomplete loss of the epidermis. • Ulceration: Discontinuity of the skin exhibiting complete loss of the epidermis and often of portions of the dermis and even subcutaneous fat. • Vacuolization: Formation of vacuoles within or adjacent to cells; often refers to basal cell-basement membrane zone area.
Blistering (Bullous) Diseases • Although vesicles and bullae (blisters) occur as secondary phenomena in a number of unrelated conditions (e.g., herpesvirus infection, spongiotic dermatitis, erythemamultiforme, and thermal burns), there exists a group of disorders in which blisters are the primary and most distinctive features. These bullous diseases, as they are called, produce visually dramatic clinical lesions and in some instances (e.g., pemphigusvulgaris) are uniformly fatal if untreated. Blisters can occur at multiple levels within the skin, and assessment of these levels is essential to formulating an accurate histologic diagnosis.
Schematic representation of sites of blister formation. A, In a subcorneal blister, the stratum corneum forms the roof of the bulla (as in impetigo or pemphigusfoliaceus) . B, In a suprabasal blister, a portion of the epidermis including the stratum corneum forms the roof (as in pemphigusvulgaris). C, In a subepidermal blister, the entire epidermis separates from the dermis (as in bullouspemphigoid and dermatitis herpetiformis).
Pemphigus is an autoimmune blistering disorder resulting from loss of the integrity of normal intercellular attachments within the epidermis and mucosal epithelium. • Although rare, its clinical consequences without treatment may be life-threatening, and its pathobiology provides important insight into the molecular mechanisms of keratinocyte adhesion. The majority of individuals who develop pemphigus are in the fourth to sixth decades of life, and men and women are affected equally. • There are four clinical and pathologic variants: (1) pemphigusvulgaris, (2) pemphigusvegetans, (3) pemphigusfoliaceus, and (4) pemphiguserythematosus.
Pemphigusvulgaris. A, Eroded plaques are formed on rupture of confluent, thin-roofed bullae, here affecting axillary skin. B, Suprabasalacantholysis results in an intraepidermal blister in which rounded (acantholytic) epidermal cells are identified (inset).
The common denominator, histologically, in all forms of pemphigus is acantholysis. • This term implies dissolution, or lysis, of the intercellular adhesion sites within a squamous epithelial surface. Acantholytic cells that are no longer attached to other epithelial cells lose their polyhedral shape and characteristically become rounded. In pemphigusvulgaris and pemphigusvegetans, acantholysis selectively involves the layer of cells immediately above the basal cell layer. (The vegetans variant has considerable overlying epidermal hyperplasia.) The suprabasalacantholytic blister that forms is characteristic of pemphigusvulgaris
Direct immunofluorescence of pemphigusvulgaris. There is deposition of immunoglobulin along the plasma membranes of epidermal keratinocytes in a fishnet-like pattern. Also note the early suprabasal separation due to loss of cell-to-cell adhesion (acantholysis
Pathogenesis. Sera from patients with pemphigus contain antibodies (IgG) to intercellular cement substance of skin and mucous membranes.111 This phenomenon is the basis for direct and indirect diagnostic immunofluorescence testing of skin and serum, respectively. Lesional sites show a characteristic netlike pattern of intercellular IgG deposits localized to sites of developed or incipient acantholysis (Fig. 25-35).
It is now known that the antibody in pemphigusvulgaris reacts with desmoglein 3, a component of the desmosomes that appear to bind keratinocytes together. • When the gene for desmoglein 3 is disrupted in genetically engineered mice, suprabasal blisters akin to pemphigus develop owing to lack of desmosome adhesion. This suggests a direct role for pemphigusautoantibodies in interfering with the function of this protein.112
Some of the acantholytic process may also be the consequence of synthesis and liberation of a serine protease (plasminogen activator) by epidermal cells, an event that is triggered by the pemphigus antibody. • The relevant antibody in pemphigusfoliaceus reacts with desmoglein 1, which is expressed in the uppermost epidermal layers, thus correlating with the characteristic subcorneal plane of blister formation in this variant.1
BULLOUS PEMPHIGOID • Originally considered to be a form of pemphigus, bullouspemphigoid has been recognized for almost four decades as a distinct and relatively common autoimmune, vesiculobullous disease. Generally affecting elderly individuals, bullouspemphigoid shows a wide range of clinical presentations, with localized to generalized cutaneous lesions and, albeit less often than in pemphigusvulgaris, involvement of mucosal surfaces.
Clinically, lesions are tense bullae, filled with clear fluid, on normal or erythematous skin • Lesions are usually up to 2 cm in diameter, but occasionally may reach 4 to 8 cm in diameter. The bullae do not rupture as easily as do the blisters seen in pemphigus and, if uncomplicated by infection, heal without scarring. • Sites of occurrence include the inner aspects of the thighs, flexor surfaces of the forearms, axillae, groin, and lower abdomen. Oral involvement is present in 10% to 15% of patients, usually after the development of cutaneous lesions. Some patients may present with urticarial plaques, with extreme associated pruritus
The separation of bullouspemphigoid from pemphigus, establishing the former as a distinctive entity, was based on the seminal observation that pemphigoid resulted from a subepidermal, nonacantholytic blister. • Early lesions show a superficial and sometimes deep perivascular infiltrate of lymphocytes and variable numbers of eosinophils, occasional neutrophils, superficial dermal edema, and associated basal cell layer vacuolization . • Eosinophils showing degranulation are typically detected directly beneath the epidermal basal cell layer. The vacuolated basal cell layer eventually gives rise to a fluid-filled blister.
Histopathology of the edge of an early lesion showing the onset of epidermal separation from the underlying dermis. Eosinophils, as well as lymphocytes and occasional neutrophils, may be intimately associated with basal cell layer destruction, creating the subepidermal cleft.
Linear deposition of complement along the dermoepidermal junction in bullouspemphigoid; the pattern has been likened to ribbon candy
Bullouspemphigoid is caused by antibodies directed against proteins at the dermal-epidermal junction. There is linear zone deposition of immunoglobulin and complement (Fig. 25-37A) at this site117 (recall that the pattern for lupus erythematosus is similar, but granular in character). • Ultrastructural studies have shown that circulating antibody reacts with antigen present in the basal cell- basement membrane attachment plaques (hemidesmosomes) (Fig. 25-37B).
The actual blister develops at the level of a narrow clear zone (lamina lucida) of the epidermal basement membrane that separates the underlying lamina densa from the plasma membrane of the basal cells. • The antigens present at these sites have been named bullouspemphigoid antigens 1 and 2, and they are now recognized as normal constituents of the hemidesmosomes that bind basal cells at the dermoepidermal junction. • In bullouspemphigoid, it is likely that the generation of autoantibodies to these basement membrane components results in the fixation of complement and subsequent tissue injury at this site through locally recruited neutrophils118 and eosinophils. Degranulatingeosinophils are often associated with necrosis of basal keratinocytes possibly related to the liberation of major basic protein from the eosinophil granule.
NONINFLAMMATORY BLISTERING DISEASES: EPIDERMOLYSIS BULLOSA, PORPHYRIA • Some primary disorders characterized by vesicles and bullae are not mediated by inflammatory mechanisms. Two such diseases are epidermolysisbullosa and porphyria. • Epidermolysisbullosa constitutes a group of disorders unified by the common link of blisters that develop at sites of pressure, rubbing, or trauma, at or soon after birth. In the simplex type, for example, degeneration of the basal cell layer of the epidermis results in clinical bullae. This form of the disease is caused by mutations in the genes encoding keratins 14 and 5. • In the junctional type, blisters occur in otherwise histologically normal skin at precisely the level of the lamina lucida. • In the scarring dystrophic types, blisters develop beneath the lamina densa, in association with rudimentary or defective anchoring fibrils. Dystrophic epidermolysisbullosa is an inherited disease resulting from mutations in the COL 7A1 gene that encodes type VII collagen. • The histologic changes are so subtle that electron microscopy may be required to differentiate among these types in clinically ambiguous settings.