Download
1 / 51
520 likes | 724 Vues
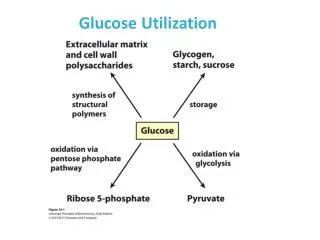
Disturbance in Glucose Utilization. Diabetes Mellitus- Gestational Diabetes- Impaired Glucose Tolerance- Hypoglycemia. Diabetes Mellitus. There are two types of diabetes mellitus: Type I, or insulin dependent (IDDM) Type II, or non-insulin dependent (NIDDM). Hanadi Baeissa.

E N D
Disturbance in Glucose Utilization Diabetes Mellitus- Gestational Diabetes- Impaired Glucose Tolerance- Hypoglycemia Hanadi Baeissa
Diabetes Mellitus • There are two types of diabetes mellitus: • Type I, or insulin dependent (IDDM) • Type II, or non-insulin dependent (NIDDM) Hanadi Baeissa
Hanadi Baeissa Hanadi Baeissa
Gestational Diabetes • A temporary type of diabetes that occurs during pregnancy Hanadi Baeissa
Impaired Glucose Tolerance • A higher than normal blood glucose level that is below the accepted value to diagnose diabetes • Diet therapy is essential for all types of disturbance in glucose utilization Hanadi Baeissa
The Goals of Diet Therapy for Diabetes • Attain and maintain desirable body weight. • Provide a normal growth rate in children and pregnant women. • Minimize glycosuria and keep the plasma glucose as near normal physiological range as possible. • Prevent and/or delay the development and/or progression of cardiovascular, renal, retinal, neurological, and other complications associated with diabetes. Hanadi Baeissa
Modify the diet as necessary for complications of diabetes and for associated diseases • Improve the overall health of the patient by attaining and maintaining an optimal nutritional status. • Provide for each patient an individualized educational and follow-up program. Hanadi Baeissa
Nutrition Guidelines • Type 1 diabetes: • Take diet history usual pattern of food intake and physical activity • Develop an individualized meal plan and schedule of insulin therapy • Emphasize the need for regular meal and snack schedule + SMBG Hanadi Baeissa
Synchronize food intake with the time of action of the insulin used, and teach patient to change dosage and time of administration to compensate for changes in the meal plan Hanadi Baeissa
Type 2 diabetes: • Take diet history usual pattern of food intake and physical activity • Aim to reduce weight • Reduce fat intake • Encourage physical activity • Emphasize the need to control BG, lipid levels and BP by dietary means, explaining how to do so • Develop an individualized meal plan Hanadi Baeissa
Diabetes in Pregnancy: A- Diabetic women who become pregnant: • Intensive therapy is indicated • SMBG must be conducted • Changing meal plan with advancing pregnancy to maintain fatal growth • Restrict energy intake for obese women (BMI > 30) • Encourage physical activity • Monitor urine for ketones Hanadi Baeissa
B- GDM • Provide adequate calories and nutrients to promote normal fetal growth • Plan meal times to maintain FBG at ≤ 95 mg/dl or 2h PPG at ≤ 120 mg/dl + SMBG • Bed time snack may be recommended to reduce risk of hypoglycemia at night • Restrict energy intake for obese women (BMI > 30) • Encourage physical activity • Monitor urine for ketones Hanadi Baeissa
Dietary management of impaired glucose tolerance Weight loss if needed Avoidance of concentrated sweets and fats Increase level of exercise Increase intake of soluble fiber incase of hyper-triglyceridemia Hanadi Baeissa
Nutritional Management of DM • Meal planning: • Balanced meals are essential • Meals should include a source of protein to slow digestion, and the increase in blood sugar • Complex carbohydrates are preferred, while simple sugars avoided • Carbohydrates should be divided carefully between meals and snacks
Some Complications of Diabetes Nutritional Management Hanadi Baeissa
Insulin Shock or Insulin Reaction & Hypoglycemia • Causes: • More insulin is injected or more oral hypoglycaemic agents are given than needed • Foods are omitted from diet • Increased physical activity • An error in insulin injection in relation to exercise Hanadi Baeissa
Symptoms: • Blood glucose decreases below acceptable level and patient sweats profusely • If not treated promptly the patient experiences : • Mental confusion and disorientation • If untreated seizures occur followed by • unconsciousness and • Death
Prevention and Management • Avoid precipitating factors • Recognize signs • Test BG • Correct hypoglycaemia • If the patient is unconscious glucagon injections must be given
Coping with acute illness • Check BG and urine ketones often • Consume 10-15 gm CHO every 1-2 hours • When vomiting, diarrhea or fever present consume liquids every 15-30 min. • Notify health care provider if cannot retain food for ≥ 4h. Hanadi Baeissa
Other complications of DM Heart disease- control fat & cholesterol intake Kidney disease- control protein intake Diabetic retinopathy- control BG and take anti-oxidants Neuropathy- control BG and take vit.B1,B6 and B12 supplement Hanadi Baeissa
Coping with gastroparesis • Give drugs to increase GI motility • Correct hyperglycemia if present • Keep record for food, BG, and symptoms to fit insulin to peak absorption time • Use short and ultra-short insulin • Decrease fat intake Hanadi Baeissa
Decrease intake of high fiber food • Give small frequent meals • Chew well • Maintain upright posture for 30-60 min after meal Hanadi Baeissa
Role of the nurse in nutritional management of diabetes Review previous history and diet Give positive verbal reinforcement for any attempt at control Identify areas of strength for positive reinforcement and areas of need for referral or personal assistance Assess the patient’s knowledge about his/her condition, and explain appropriate action in various situations Hanadi Baeissa
Reactive Hypoglycaemia • Postprandial • Second most common type of hypoglycaemia • Caused by exaggerated insulin release following a meal leading to transient hypoglycaemia. • Glucose returns to normal without food. Hanadi Baeissa
Dietary management of reactive hypoglycemia • Limit the intake of simple sugars, and conc. Sweets • Emphasize complex carbohydrates • Eat small frequent meals and snacks (every 2 to 3 hours) • Include a protein source with meals and snacks • Restrict intake of caffeine Hanadi Baeissa
Factors to consider: • Weight and height • Caloric needs • Division into protein, carbohydrate and fat • Division into meals and snacks • Limitations (modifications for special condition) • Need for insulin • Individual food habits • Family food budget Hanadi Baeissa
Weight and height Hanadi Baeissa
Determination of caloric needs • For adults • Basal calories equals desirable body weight (Ib.) x 10, or (Kgx 22) • Add activity calories • Sedentary equals desirable body weight (Ib.) x 3, or ( Kg x 6.6) • Moderate equals desirable body weight (Ib.) x 5, or (Kg x11) • Strenuous equals desirable body weight (Ib.) x 10, or (Kgx22) Hanadi Baeissa
Add calories for indicated weight gain, growth (pregnant women), or lactation • Subtract calories for indicated weight loss Hanadi Baeissa
For children • Children vary markedly in their caloric needs depending on rate of growth and level of activity • Estimate caloric requirement from chart of Recommended Daily Dietary Allowances • Adjust caloric intake as needed to maintain normal rate of growth Hanadi Baeissa
Determination of grams of protein, carbohydrate and fat • Protein:20% of total calories for growing children and pregnant women, minimum of 0.5 gm per Ib.(1.1 gm/Kg)desirable body weight for other adults • Carbohydrate:from 50-70% of non-protein calories • Fat:from 30-50% of non-protein calories Hanadi Baeissa
Example for diet order of 2000 kcal /day • Protein:2000x0.15=300 kcal ÷4(kcal/g)=75g • Carbohydrate:2000x0.6=1200 kcal ÷ 4(kcal/g)=300g • Fat:2000x0.25=500 kcal ÷ 9(kcal/g)=55g
Suggested division into meals and snacks • Meals usually contain 2/10 to 4/10 of the calories and carbohydrate, and snacks usually contain 1/10 of the calories and carbohydrate Hanadi Baeissa
b. In the non-insulin dependent individual, food is usually divided into three meals per day. In the insulin dependent individual, food is usually divided into three meals and a bedtime snack and occasionally a mid-afternoon and/or mid-morning snack, depending on plasma glucose levels
Limitations (modifications for special conditions) • Protein • Saturated fat and/or cholesterol • Sodium • Potassium • other Hanadi Baeissa
The GI Factor The increase in the area under the blood glucose curve after the ingestion of 50 gm of carbohydrate in the test food compared to the area under the curve when 50 gm of glucose or white bread is taken Hanadi Baeissa