Download
1 / 52
520 likes | 635 Vues
This text presents a comprehensive overview of HIV drug development, focusing on the challenges posed by resistance to antiretroviral (ARV) drugs and the evolving landscape since the introduction of AZT in 1987. It highlights the importance of combination therapy (HAART) and addresses the need for new ARV agents with improved efficacy, tolerability, and compliance. The discussion also emphasizes the role of co-receptors in HIV infection and the necessity for innovative treatment approaches in both developed and developing countries to combat the HIV pandemic effectively.

E N D
Drug Development in HIV Michael Zaiac New Product Development 25/11/05
Contents • Background-Setting the scene • Co receptors and HIV • Co-receptor tropism • Co-receptors as targets • Philanthropy • Summary
No Sign of Pandemic Abating Issues • No vaccines on horizon • Resistance to ARV drugs increasing • Western World - re-invigorate public health campaigns - new ARV to address resistance & compliance • Developing World - ARV to break infection cycle - healthcare infrastructure & public education - economic stability - global political leadership
Eastern Europe & Central Asia 1.4 million 210,00060,000 North America and Western/Central Europe 1.6 million 64,000 23,000 North Africa & Middle East 540,000 92,00028,000 Asia 8.2 million 1.2 million540,000 Caribbean 440,000 53,000 36,000 Sub-Saharan Africa 25.4 million 3.1 million2.3 million Latin America 1.7 million 240,00095,000 Oceania 35,000 5000700 Total living cases: 39.4 million New cases, 2004: 4.9 million AIDS Deaths, 2004: 3.1 million Estimated Number of People Living With HIV, by Region in 2004 UNAIDS/WHO, 2005
Goals of Antiretroviral Treatment 1. Prevention of progressive immunodeficiency;potential maintenance or reconstruction of a normal immune system 2. Control of viral replication and mutation; reduceviral burden Delayed progression to AIDS and prolongation of life Decreased risk of selection of resistant virus
Anti-Retroviral Therapy • Explosion in HIV research since 1980 & AZT in 1987 • But…HIV challenging target - obligate parasite, so few viral targets - high mutation rate & genetic plasticity • > 20 approved agents but only 4 targets • Combination therapy (at least 3 agents) = HAART introduced in 1995 - reduce propensity to resistance
Genetic Plasticity • 109 new virions produced daily • One mutation during every replication cycle per cellular genome • Genetic plasticity enables HIV to: - evade immune system - develop resistance to ARV - produce mutants with different ‘fitness’ • Multiple strains co-exist & are archived in patients’ immune cells
Emergence of HIV Resistance Total plasma HIV RNA Wild-type (WT) HIV RNA Mutant HIV RNA Plasma HIV RNA Time Receiving Treatment Havlir. Ann Int Med 1996:124:984.
Class Drug Nucleoside/tide Reverse Transcriptase Inhibitors Zidovudine, Zalcitabine, Didanosine/EC, Stavudine/XR, Combivir, Trizivir, Lamivudine, Abacavir, Tenofovir Non-Nucleoside Reverse Transcriptase Inhibitors Efavirenz, Delavirdine, Nevirapine Enfuvirtide Fusion Inhibitors Protease Inhibitors Saquinavir, Indinavir, Ritonavir, Nelfinavir, Amprenavir, Lopinavir/Ritonavir, Atazanavir Approved ARV Agents
Problems with HAART • HAART = HIV chronic disease & saves lives • But… most agents designed for acute disease • HAART has considerable drawbacks: - toxicity & side effects - drug interactions - high pill burden & inconvenient dosing • Tox. & inconvenient dosing reduce compliance • Resistance emerges within 6 months to 5 years - up to 27% of newly diagnosed HIV is resistant
= compliance & durability Requirements on HIV medicines Ideal features of an antiretroviral agent: - low dose - convenient regimen - better toleration - non cross resistant - new mechanisms & targets - low COG
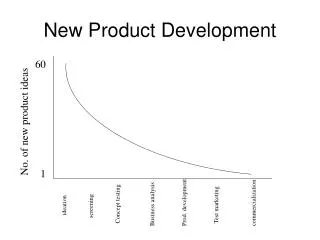
Attrition on the R&D Process 1 Medicine
Years 0 1 2 3 4 5 6 7 8 9 Candidate attrition 25 animal toxicity, chemical stability, superior compound human PK, tolerability, formulation 12 No. candidates Efficacy, safety, differentiation, Dose, c.o.g. long-term safety non-approval 4 0 Preclin. Phase I Phase II Phase III Registration
0 1 2 3 4 5 6 7 8 9 10 New medicine development Medicine Development Costs Time/Cost of Medicine Development Launch £450 million File 500 400 £280 million Phase III 300 £200 million Cumulative costs £M Phase I 200 Phase II £70 million 100 £30 million 0 Years
CCR5 and CXCR4 Co-Receptors:HIV Binding and Entry CD4 CXCR4 CCR5 T-Cell Surface
HIV-1 Envelope Glycoproteins HIV-1 gp41 gp120 HIV-1 Envelope Glycoprotein CD4 CCR5 T-Cell Surface
Binding of the gp120 Subunit of the HIV-1 Envelope Glycoprotein to CD4 HIV-1 gp41 gp120 CD4 CCR5 T-Cell Surface
Conformational Change Exposes theCo-Receptor Binding Site in gp120 HIV-1 gp41 gp120 CD4 CCR5 T-Cell Surface
Conformational Change Allows gp120 to Bind to the Co-Receptor HIV-1 gp41 gp120 CD4 CCR5 T-Cell Surface
Fusion of HIV and T-Cell Membranes HIV-1 RNA HIV-1 HIV-1 Nucleocapsid T-Cell Surface
HIV-1 Tropism Assays:MT-2 Cell Assay • Indirect measure of co-receptor use • Depends on the presence of X4 or R5/X4 isolates • Uses viral stocks from stimulated patient lymphocytes • Results are reader dependent and involve the interpretation of typical cytopathic changes • Limitations • HIV derived from stimulated lymphocytes may differ from that of plasma virus • Qualitative nature of the assay result • Detection of CXCR4 only Moore JP, et al. AIDS Res Hum Retroviruses. 2004;20:111-126. DAIDS Virology Manual for HIV Laboratories. 1997. Publication NIH-97-3828. U.S. Department of Health and Human Services, Washington, DC.
MT2 cell assay Syncytium Formation in MT-2 Cells • Prior to the discovery of the role that CCR5 and CXCR4 play in viral entry, viruses were characterized by ability to infect T-cells and cause syncytium formation • MT-2 cell lines were used • MT-2 cells express only CXCR4 • Syncytium inducing (SI) • Changed to CXCR4-using virus • Non-syncytium inducing (NSI) • Changed to CCR5-using virus Schuitemaker H, et al. J Virol. 1991;65:356-363. Japour AJ. J Clin Microbiol. 1994;32:2291-2294.
HIV-1 Tropism Assays:Recombinant Phenotypic Assays • Direct measure of co-receptor use • Infect engineered cell lines to determine co-receptor utilization • Obtained by RT-PCR from patient plasma sample • Virus stocks pseudotyped with envelope sequences derived from patient plasma samples • Limitations • >500 copies/mL • May fail to detect X4 when X4 virus constitutes <10% of the viral population • Sequence variation may result in assay failure Coakley E, et al. Curr Opin Infect Dis. 2005;18:9-15.
CD4 + CXCR4 + HIV env expression vector HIV genomic luc vector + Infection Transfection Pseudovirus CD4 + CCR5 + HIV entry cell assay Adapted from Petropoulos CJ et al. Antimicrob Agents Chemother 2000;44:920-8.
R5 Infection R5 and X4 Variants:HIV Disease Progression Absolute Viral Load R5 X4 Limit of Detection Weeks Years Time After HIV Transmission Kuhmann SE, et al. J Viral Entry. 2005;1:4-16. Moore JP, et al. AIDS Res Hum Retroviruses. 2004;20:111-126.
R5 Infection R5 Infection R5 and X4 Variants:HIV Disease Progression Absolute Viral Load R5 X4 Limit of Detection X4 Weeks Years Time After HIV Transmission Kuhmann SE, et al. J Viral Entry. 2005;1:4-16. Moore JP, et al. AIDS Res Hum Retroviruses. 2004;20:111-126.
R5 Infection R5 Infection R5 and X4 Variants:HIV Disease Progression R5 + X4 Infection Absolute Viral Load R5 X4 X4 Limit of Detection Weeks Years Time After HIV Transmission Kuhmann SE, et al. J Viral Entry. 2005;1:4-16. Moore JP, et al. AIDS Res Hum Retroviruses. 2004;20:111-126.
R5 and X4 Viruses TargetDifferent Subsets of CD4+ T-Cells R5 Infection (common, early) Naïve T-Cells Relative CD4 Cell Counts Memory T-Cells Time (y) R5 viruses target memory T-cells (eg, GALT) Naïve T-cells become targets once activated to the memory phenotype Douek DC, et al. Ann Rev Immunol. 2003;21:265-304. Kuhmann SE, et al. J Viral Entry. 2005;1:4-16.
X4 Infection (very rare) Memory T-Cells Relative CD4 Cell Counts Naïve T-Cells Time (y) X4 viruses target naive T-cells (eg, thymus) CXCR4 expression on some memory cells makes them targets R5 and X4 Viruses TargetDifferent Subsets of CD4+ T-Cells R5 Infection (common, early) Naïve T-Cells Relative CD4 Cell Counts Memory T-Cells Time (y) R5 viruses target memory T-cells (eg, GALT) Naïve T-cells become targets once activated to the memory phenotype Douek DC, et al. Ann Rev Immunol. 2003;21:265-304. Kuhmann SE, et al. J Viral Entry. 2005;1:4-16.
Will a CCR5 Antagonist Drive the Emergence of X4 Viruses In Vivo? Scenario 1 CCR5 Antagonist R5 Absolute Viral Load X4 Threshold of Detection X4 Time (days) R5 viruses remain suppressed X4 viruses do not expand
Scenario 2 CCR5 Antagonist R5 X4 Viral Load X4 Threshold of Detection Time (days) R5 viruses remain suppressed Sustained, possible reciprocal expansion of X4 virus pool Will a CCR5 Antagonist Drive the Emergence of X4 Viruses In Vivo? Scenario 1 CCR5 Antagonist R5 Absolute Viral Load X4 Threshold of Detection X4 Time (days) R5 viruses remain suppressed X4 viruses do not expand
Scenario 3:Partial Expansion of the X4 Virus Pool Scenario 3 CCR5 Antagonist R5 X4 Absolute Viral Load X4 Threshold of Detection Time (days) R5 viruses remain suppressed Sustained, partial expansion of X4 virus pool
Prevalence ofHIV Co-Receptor Usage 1Fätkenheuer G, et al. Nat Med. 2005;11:1170-1172. 2Brumme ZL, et al. J Infect Dis. 2005;192:466-474. 3Moyle GJ, et al. J Infect Dis. 2005;191:866-872. 4Demarest J, et al. 44th ICAAC. Washington, DC, 2004. Abstract H-1136. 5Whitcomb JM, et al. 10th CROI. Boston, 2003. Abstract 557.
Δ32 CCR5 WT CCR5 < 1.5% < 20% ~ 80% Delayed progression Normal progression (Essentially) no progression 100 80 Genotype +/+ Genotype +/∆32 60 % AIDS free 40 n = 39 20 n = 110 0 0 2 4 6 8 10 12 14 16 18 20 Years since seroconversion Δ32 inhibition of coreceptor-mediated entry Lui R, et al.Cell 1996; 86:367–377.Samson M, et al. Nature 1996; 382:722–725.Dean M,et al. Science 1996; 273:1856–1862. Huang Y, et al.Nature Med 1996; 2:1240–1243.Michael NL, et al. Nature Med 1997; 3:1160–1162.Eugen-Olsen J,et al.AIDS 1997; 11:305–310.
Drug development Designer Drugs SAR HIV inhibition High-throughputin vitro testing Normalfunction CCR5 CXCR4 crystallography
Unknown effects of entry inhibitors Normal Function natural ligand allosteric inhibition by drug Internalisationof receptor ? Normal function ? Internalisation of receptor Viral mutations overcome
some Co-receptor antagonists have fallen by the wayside SCH-C QT AMD-3100 cardiac abnormalities but stem cell mobilization ALX 404 C no oral formulation TAK 779 toxicity at injection sites Aplaviroc hepatic side effects
Using CCR 5 antagonists Tropism shift
Impact of Current Antiretroviral Agents on R5 and X4 Virus Dynamics • In 3 cohorts, patients on HAART who were X4 or X4/R5 tropic showed a:1-4 • Preferential suppression of X4 • Shift from X4 to R5 • Loss of X4 from T-cell reservoirs in some cases • Treatment experience associated with greater risk of X4 in some cohorts5 • Acquisition of X4 virus in 8 persons homozygous for D326 • Rapid initial CD4 decline • Established wide variation in viral load “set point” • Rapid progression not invariable • Suggested behavior of X4 virus less pathogenic than in late stage • Is X4 cause or effect of progression? 1Skrabel K, et al. AIDS. 2003;107:431-438. 2Philpott S, et al. J Clin Invest. 2001;107:451-458. 3Equils O, et al. J Infect Dis. 2000;182:751-757. 4Van Rij RP, et al. J Virol. 2000;76:3054-3058. 5Demarest J, et al. 44th ICAAC. Washington, DC, 2004. Abstract H-1136. 6Sheppard HW, et al. AIDS. 2002;29:307-313.
CCR5 Antagonists:Potential Advantages • Inhibit entry of HIV-1 into host cells • Activity against viral strains resistant to current agents • Human protein target versus viral gene target • Extracellular mechanism of action
Challenges in CCR5 Antagonist Use • Utility may be related to disease stage, rather than treatment experience • Higher prevalence of X4 virus in patients with advanced disease • Trends toward later initiation of therapy may limit utility of CCR5 antagonists • Clinical trials underway to address: • Long-term safety of CCR5 inhibition • Frequency/risk/implications of X4 emergence/unmasking • Risk/benefit in patients with mixed infection • Possible need for laboratory monitoring of viral tropism?
Possible scenarios • Noninferiority proven • New class Unknown risks • Laboratory issues • ‘Superiority’ proven • Salvage – as part of last viable regimen • NRTI sparing • Substitution studies
Diflucan Partnership Program • Donation of Diflucan (fluconazole) and training of health care providers • 22 countries (915+facilities) in Africa, Asia and Caribbean participating • 67,000 patients treated for HIV-related fungal opportunistic infections • More than 18,000 health care professionals trained The Diflucan Partnership is “the first of, we hope, many other successful public/private partnerships initiated by parties who have demonstrated that they care enough to act.” — Dr. Manto Tshabalala-Msimang, Minister of Health, South Africa
International Trachoma Initiative • Public-private partnership focused on eliminating blinding trachoma • The world’s leading cause of preventable blindness • ITI now in place in 9 countries in Africa and Asia • 90% reduction in prevalence in Morocco • 50% in Tanzania • 75% in Vietnam • Donated $225 million worth of Zithromax • 10 million antibiotic treatments to date
Infectious Diseases Institute • $11 million commitment to fund regional Center of Excellence for HIV/AIDS treatment and training at Makerere University in Kampala • Extensive, one-month HIV training program for 150 physicians each year in Uganda and the region • Care and treatment for more than 50,000 patients annually • Construction of facility completed March 2004