Diagnostic Methods for Peripheral Artery Diseases
340 likes | 427 Vues
Learn about diagnostic methods, symptoms, and treatments for peripheral artery diseases (PAD) affecting limbs. Understand PAD prevalence, risk factors, classification, and treatment options including revascularization and lifestyle changes.

Diagnostic Methods for Peripheral Artery Diseases
E N D
Presentation Transcript
Peripheralarterydiseases Jakub Honěk Kardiologická klinika 2.LF UK a FN Motol
Diagnostic methods • Peripheral artery diseases (limb ischemia) • Chronic PAD • Acute limb ischemia • Compressive syndromes • Vasospastic disorders • Specific localization of PAD • Vasculitis
Diagnosticmethods • Medical history, physical examination • Measurement of peripheral arterial pressure (+ ABI, TBI) at rest, after exercise • Plethysmographic examination • TcpO2 • Teadmill walking test • Color duplex sonography • X-ray based methods - DSA, CTA, MRA
Peripheral BP (mmHg)ankle >100…, 50-100 … (claudication), <50 … (criticalischemia)toe < 30 … (criticalischemia)
tcpO2 • Testing peripheral skin perfusion on the capillary level; testing skin nutrition • Closely corresponds to the capillary pressure of O2 →To determine the degree of perfusion (ischemia),evaluate the effectiveness of revascularization,determineamputation line,predict effectofhyperbaric oxygen therapy
tcpO2 (transkutánní měření parciálního tlaku kyslíku ve tkáni)
Plethysmography • Photopletysmography- emitted infrared light is reflected Hb, while in tissues without Hb is absorbed or released (decay curve) →detection of acral blood circulation disorders; examinationpatientswith DM (mediocalcinosis); dif.dg. TOS; cooling test
Duplex ultrasound Bifurcation Atherosclerotic plaque
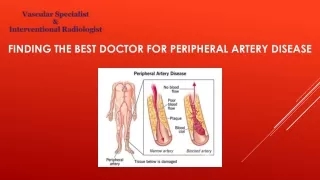
Peripheralarterydiseases (PAD) • Peripheral artery disease (PAD) generally refers to a disorder that obstructs the blood supply to the lower or upper extremities • 90-95 % atherosclerosis • 5-10% thrombosis, embolism, vasculitis, fibromuscular dysplasia, entrapment • Impcacton qualityoflife + mortality (cardiovascular) • > 50% patients with PAD at the same time suffer from coronary atherosclerosis, 15-40% and carotid atherosclerosis
Modifiable risk factors(atherosclerosis) • Cigarette smoking • Dyslipidemia • Diabetes • Arterial hypertension
Less frequent causes of PAD • Coarctationofthe aorta • Vasculitides • Tromboangiitisobliterans (Buergersdisease) • Peripheralembolisationfromvariousorigins • Entrapmentsy AP • Cysticadventitialdegeneration AP • fibromusculardysplasia • Iliacarteryendofibrosisofcyclists • Primaryvasculartumors • Compression (tumorsetc.) • Vascular trauma • Iatrogenic vascular disease (percutaneous and surgical procedures) • Irradiationarterialdisease
Symptoms • Chronic disease • Claudication – muscle ischemia • Site of stenosis correlates with site of pain • intermittent claudication – on exertion • Critical limb ischemia • Acute vs. chronic • Limb/life threatening disease • paresthesia, pain at rest
Rutheford Peripheralarterialdisease - classification Fontain
Intermittentclaudication • Metabolic demands of muscle not met during exercise • Higher demand (muscle work) • Flow limitation (pressure gradient) • Impaired vasomotion • Steal syndrome • Pain one level bellow stenosis • Tredmill test – determines walking capacity, ABI after exercise (pain + 25% decrease in ABI confirms diagnosis)
Acute limb ischemia • ←70-80% embolicclosure (sudden PAD) • ←30-20% thrombotic occlusion (mostlythrombus on rupturedplaque - acute worsening of existing PAD) • Clinicalpicture- incomplete X completeischemicsy (6Ps) Pain Paleness Pulselessness Paresthesias Paralysis Prostration
Treatmentofacute limb ischemia • i.v. Heparin, i.v. analgesics → urgent revascularization (DSA) • Surgical embolectomy- pelvic arteries, arm and forearm arteries • Endovascular therapy- LTL, thrombus aspiration, mechanical revascularization • Combination of both
Treatmentofchronic PAD • Cardiovascular mortality prevention • antiplatelet drugs (ASA) • risk factor modification (statins!, antihypertensives…) • Lifestyle changes, exercise • QoL improvement – control of claudications • Vasocative agents (cilostazol 2x100 mg, naftidrofuryl 3x200 mg) • Few clinical data supporting effectivity of vasoactive drugs • Prostanoids – critical limb ischemia • Exercise • Revascularization
Treatmentofchronic PAD • Methods of revascularization • Endovascular (percutaneous, invasive) • PTA (DEB; BMS, DES); stentgrafts; SIR; thrombolysis • surgery • bypass, endarterectomy, amputation • Stimulation of angiogenesis(stem cells) ?? • Lumbar sympathectomy
Lerich`s syndrome(total subrenal occlusion of aorta) • Claudication in buttocks, hypotrophy of thighs, impotence in ♂ • Treatment - aorto-bifemoral bypass
Compressivesyndromes • compressionof arteries, veins, nerves (or all 3 systems) – - anatomical structures (costoclavicular sy) - anatomical anomalies (cervical rib) - different course (medial course of a.poplitea)
Thoracicoutlet syndrome • compression of neurovascular bundle • between scalenous muscles • In costoclavicular space • at the insertion of m. pectoralis minor
Thoracicoutlet syndrome • symptomatology - neurogenic 95% - arterial 3-5% - venous 2% • symptoms-carrying an umbrella, washing windows, painting walls, driving… • Therapy - rehabilitation→ improvements up to 70% within a few months - surgical(resection of the first rib) in severe disability
Costoclavicular syndrome • represents 80% of all TOS • compression of neurovascular bundle (a.,v., n.) between the clavicle and the first rib
Entrapment syndrome ofpoplitealartery • the most common cause of limb ischemia in patients under 35 years • ← abnormal course of PA • ← non-physiological hypertrophy of the surrounding structures • ← presence of abnormal structures (fibrous bands) dg. MR- relation of vascular bundle with the surrounding muscle or connective structures th. surgery (LTL and PTA only to improve the outflow tract for surgical reconstruction)
Specificlocalizationof PAD • Visceral ischemia • Carotid artery disease • Renal arteries
Vasospasticdisorders • Usually reversible localized narrowing of smallarteries • primary disorders do not lead to trophic changes • Raynaudsphenomenon • Primary: morbusRaynaud- etiology is not clearly known, suspected failure of regulation at the level of the terminal vascular bed • Secondary: Raynaud´ssyndrome – secondary to another underlying disease
Raynaud's phenomenon • 1st phase: ischemia → morbidly pale fingers, paresthesia, 5-60 min. • 2nd phase:stasis of blood in the capillaries and veins → cyanosis • 3rd phase: reactive hyperemia → reddening
PrimaryRaynaud's syndrome • paroxysmal character, symmetrically, except thumb • women 5x more often than men • ♀ between puberty and 30 years old, after pregnancy or menopause problems often disappear
SecondaryRaynaud'ssyndrome • Connective tissue disorders • SLE, RA, sclerodermia… • PAD • Buergers disease, atherosclerosis, TOS… • Drugs • Occupational diseases • Vibration – drilling, cold exposure • Malignancy • Other causes
Takehomemessages • PAD – occlusive diseases of peripheral (limb) arteries • 90% atherosclerosis (modfiable risk factors – smoking!, CV mortality) • Imaging – DUS, CT (MR), angiography • Chronic PAD (claudication, crtitical limb ischemia) vs. Acute limb ischemia • Treatment – CV risk modification + revascularization (endovascular, surgical) • Many other disorders (vasculitides, compression sy., vasospastic disorders…)