Peripheral Vascular Diseases
Peripheral Vascular Diseases. Howard Sacher, D.O Long Island Cardiology and Internal Medicine. Significance of Peripheral Vascular Disease. Recognition and management of diseases of the peripheral arteries and veins should be a legitimate part of cardiovascular practice


Peripheral Vascular Diseases
E N D
Presentation Transcript
Peripheral Vascular Diseases Howard Sacher, D.O Long Island Cardiology and Internal Medicine
Significance of Peripheral Vascular Disease • Recognition and management of diseases of the peripheral arteries and veins should be a legitimate part of cardiovascular practice • These disorders so commonly coexist with, occur as complications of, and at times are the presenting clinical manifestation of cardiac disease. • In our aging population, atherosclerotic occlusive peripheral arterial disease (OPAD) is common.
OPAD is present to some degree in at least half of patients with coronary artery disease. • When symptomatic, chronic OPAD presents with intermittent claudication. • With progression of occlusive arterial disease and the development of more severe ischemia, there is pain at rest—'ischemic rest pain.'
Physically Examining the Patient • Pulsation • Bruits • Elevation-Dependency Tests • Ischemic Ulceration present?
Pulsation • Examination should include palpation and characterization of the pulsation of the upper and lower extremity arteries and the cervical carotid. • One of the best clinical criteria indicative of OPAD is an absent posterior tibial artery pulse. For illustrations of examination methods
Bruits • Most often, bruits due to occlusive arterial disease are systolic in timing. • Useful bedside point: a bruit that extends into diastole indicates a stenosis severe enough (usually 80% or greater) to produce a gradient in diastole
Elevation-Dependency Tests • Elevation-dependency tests are also useful in evaluating the person with occlusive peripheral arterial disease
Presence of Ischemic Ulcers • Ischemic ulcers are extremely painful, are located most often on the toes or heel, can occur at any site of trauma to an ischemic limb, and can usually be readily distinguished from other leg and foot ulcers
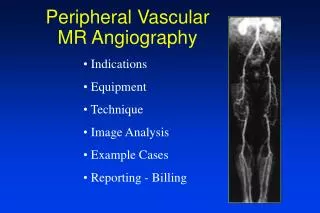
Noninvasive Evaluation • Ankle:Brachial index • Duplex scan with color flow Doppler • Magnetic Resonance Angiography
But Invasive test is the Gold Standard • Arteriography remains the best means of evaluating OPAD when restoration of pulsatile flow is being considered
MRA gives us a good view of vasculature with the use of gadalidium contrast
Gold standard for evaluation of the patency is with an angiogram • Look at this high grade stenosis of the left common iliac
Along with with an angiogram, the interventionalist can also perform a Percutanous Transluminal Angioplasty (PTA) using a balloon and and a stent
Thromboangitis Obliterans • Burger’s Disease • Primarily effects smokers • Complete obliteration of the small to medium size vessels • Px is poor • Tx is to stop smoking
Acute Peripheral Arterial Occlusion • Classic Occlusion • Acute peripheral arterial occlusion may present classically with the 5 Ps • Pain • Pallor • Paresthesia • Paralysis • Pulselessness Or may be more subtle.
Aortagram shows a complete occlusion of the left subclavian in the thoracic outlet –Thoracic Outlet Compression
Raynaud’s Phenomenon is also associated with ispilateral thoracic compression
Atheroembolism • Management includes removal of the source of the debris. Anticoagulant therapy with either heparin or warfarin and thrombolytic therapy should be avoided, while treatment with aspirin and/or dipyridamole has been reported to improve a limited number of patients.
Ergotism • The manifestations of ergotism are usually symmetric and vary from Raynaud's phenomenon to claudication or even acute arterial occlusion. • Treatment with intravenous sodium nitroprusside in addition to discontinuing ergot preparation will relieve the arterial insufficiency
Aneurysmal Disease • Arterial aneurysms are more common in males 60 years of age or older • Coronary and cerebral arterial disease are frequent comorbid conditions • Abdominal Aortic Aneurysm (AAA) needs to be kept in mind as a possible cause of unexplained abdominal, flank, or back pain in a man with an elevated sedimentation rate, a tender pulsatile abdominal mass, and rarely, weight loss or ureteral obstruction. • CT and MRI are useful to differentiate a leaking aneurysm from inflammatory AAA.
Most thoracic aortic aneurysms today are atherosclerotic • But other causes such as sudden deceleration are also important. • Given findings consistent with incomplete aortic rupture, aortography is indicated. • Surgical repair is indicated in the case of incomplete rupture or post-traumatic aneurysm in persons who are suitable surgical candidates.
Ultrasound is a reliable diagnostic technique for abdominal aortic aneurysm • Screening of elderly patients during echocardiography has a significant yield in discovering occult abdominal aortic aneurysm • In a good-risk patient, elective surgical treatment is advisable for aneurysms more than 4.5 cm in diameter • Because of the continued high mortality of ruptured abdominal aortic aneurysm, an aggressive approach to diagnosis and treatment is appropriate