Download
1 / 34
460 likes | 1.93k Vues
Peripheral Vascular MR Angiography. Indications Equipment Technique Image Analysis Example Cases Reporting - Billing. Thank You. Yi Wang, PhD Qian Dong, MD Richard Watts, PhD Jim Meaney, MD Priscilla Winchester, MD Vince Ho, MD Neil Khilnani, MD Tom Chenevert, PhD

E N D
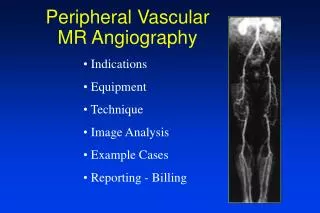
Peripheral Vascular MR Angiography • Indications • Equipment • Technique • Image Analysis • Example Cases • Reporting - Billing
Thank You Yi Wang, PhD Qian Dong, MD Richard Watts, PhD Jim Meaney, MD Priscilla Winchester, MD Vince Ho, MD Neil Khilnani, MD Tom Chenevert, PhD David Trost, MD Craig Kent, MD Bernie Redd, MD
Indications: • Intermittent Claudication • Non-healing ulcer • Post bypass graft • Aneurysm • Pre free-flap • Pediatric
Indications for MRA • Difficult access • Renal insufficiency Cr > 2.0 • Allergy to iodinated contrast • Patient refuses conventional angiography
Advantages of MRA • No nephrotoxicity • Allergic reactions rare • 3D • Anatomy and Physiology • High Accuracy • Affordable (reimbursement = $1159)
Advantages of Gadolinium • No pulsatility artifact • No slice misregistration • No in-plane saturation • High resolution (1.8 x 1.6 x 2.6 mm) • Fast
Equipment for Peripheral MRA • Magnet: • 1.5 Tesla high SNR • 0.5 Tesla requires more Gd • High performance gradients • Coil: body and head coil • Injector vs hand injection • Foam and straps
Table Positioning Pole PVC tubing 2 inch diameter 3-4 meters long holes at 36 or 40 cm spacings
Technique: younger vs older Young Adult Older patient 2D TOF Tech (30 years old) 2D TOF Radiologist (41 years old) 2D TOF: 1 hour 3D Gd MRA: 87 seconds
Technique • Pediatric – Young Adult (fast flow) • Head or extermity coil • 2D time-of-flight • Gd almost never necessary • Gating +/- • Older Patients (slow flow) • Head coil • 2D projection MRA of ankle-feet • Body coil • 3D Bolus chase MRA: Renals distal calf • 3D phase contrast of renal arteries
3 Critical Details • Positioning • Bolus timing • Subtraction Unsubtracted Subtracted
Bolus Chase MRA Technique • 2D Projection MRA (timing): 1 min • Floating Table 7 min • Sag Loc 1 min • Axial Loc 3 min • Cor 3D-Gd-MRA • Pre 1.5 min • During 1.5 min • 3D phase contrast (renals) 7 min Total Imaging Time 15 min Total Exam Time <1 hr
2D Projection MRA: ankle-feet Complex subtraction Raw image Left Right Coronal T1
2D Projection MRA: + complex subtraction Ankles Knee
2D Projection MRA (Left foot) 20.3 sec 32.5 sec 72.7 sec 24.4 sec 28.4 sec • Time to fill distal station = 24 seconds • Time to fill pelvis = 2/3 (24 sec) = 16 sec • Time for venous contamination = 60 sec
6 6 Calculation of Bolus-Chase Injection Timing Parameters Time to venous contamination = 60 seconds Time to fill pelvis = 16 seconds Centers of k-space scan delay 6 Station 1 = pelvis Station 2 = thigh Station 3 = calf 65 45 10 30 0
Bolus Chase MRA Preparations • level legs • secure feet with curlex • determine length of stations • landmark above umbilicus
Position for Overlap at Critical Sites Overlap Trifurcation Overlap Common Femoral Bifurcation
2D TOF Internal iliac P 60 A 25 Common femoral Popliteal P 45 A 30 Ankle P 20 Bolus Chase Positioning
A 24.8 P 60.2 Selecting Imaging Parameters Slice thickness = 3 (2-5) mm # of slices = 28 (20-40) Frequency = 256 Phase = 160 (128-256) Phase FOV = 0.8 (1-0.6) Bandwidth = 31 (31 or 62)
3D Gadolinium Bolus Chase MRA • Breathhold 1st station • Use oxygen liberally • Scan delay ~ 10 sec
Image Post Processing • Digital subtraction: pre from post • Complex Fourier Subtraction • Do not subtract MIPs • MIP subtracted source images • Reformat into lateral & oblique projections • Subvolume MIPs for selected regions • renal arteries • mesenteric arteries • common femoral bifurcations • regions of greatest interest • Examine pulsatility artifact on 2D TOF images
Oblique views obtained by reformatting data on computer even after patient leaves Oblique MIP Coronal MIP
Popliteal Artery Aneurysm • Male>>> female • Risk of complications • thrombosis => high • emboli => high • rupture => low • Associated with other aneurysms
Patient could not straighter knee 2D Projection MRA
Peripheral Vascular MRA Year # Patients Technique Sensitivity Specificity Owen (NEJM) 1992 23 2D TOF superior to DSA Baum (JAMA) 1995 155 2D TOF 82 84 Prince (Radiology) 1995 43 3D Gd 94 98 Snidow (Radiology) 1996 32 3D Gd 100 98 Hany (Radiology) 1997 39 3D Gd 93-96 96-100 Ho (Radiology) 1998 28 Bolus chase 93 98 Meaney (Radiology) 1998 20 Bolus Chase 81-89 91-95 Yamashita (JMRI) 1998 20 3D Gd 96 83 Lee (Radiology) 1998 23 2D Gd 94 91 Winchester (JMRI) 1998 22 2D Gd 90 98 Link (Radiology) 1999 67 3D Gd 100 83 (post stent)
Useful Descriptors DescriptorMeaning • Occluded • Severe stenosis > 75% narrowing • Moderate stenosis 50-75% • Mild stenosis < 50% narrowing • Normal normal • Widely patent wide open: +/- tortuosity +/- atherosclerotic irregularity • Ectatic diameter < 50% more than normal • Aneurysmal diameter > 50% over normal
Useless Descriptors DescriptorMeaning • Stenotic “I think there is a stenosis” • Patent “I see the artery”
MRA Summary • No Ionizing Radiation • No Contrast Injection necessary • If Contrast No nephrotoxicity • Reformat to obtain an view • Anatomy and Physiology • High Accuracy • Tremendous Future