Download
1 / 37
480 likes | 865 Vues
Management of First-time Anterior Shoulder Dislocations. Natasha Holder. 19 M with Left Shoulder Pain. Healthy, No medications, Right Hand dominant Presents to ER with left shoulder pain after being checked from behind while playing hockey. Management?.

E N D
Management of First-time Anterior Shoulder Dislocations Natasha Holder
19 M with Left Shoulder Pain • Healthy, No medications, Right Hand dominant • Presents to ER with left shoulder pain after being checked from behind while playing hockey
Management of First-time Anterior Shoulder Dislocations Natasha Holder
Objectives • Does a high-risk group exist? • If so, what are the risk factors? • What is the recommended treatment?
Incidence • Shoulder is the most commonly dislocated joint • Traumatic Dislocations • Anterior 96% • Posterior 2-4% • Incidence 1.7% Hovelius et al. Clin Orthop 1984; 166:127-131
Anatomic Considerations • Glenohumeral stabilization mechanisms • Static: joint conformity, negative pressure, ligamentous and capsular restraints, labrum • Dynamic: Rotator Cuff
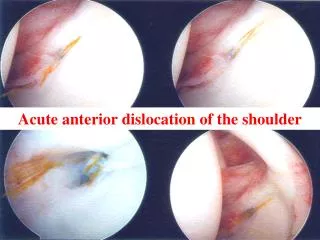
Pathology of Acute Dislocation • Taylor and Arciero • First time dislocators in the young (<24 yrs) • 97% Bankart lesion • 89% Hill-Sachs (small) • 10% Slap tear • No rotator cuff tears Taylor et al. Am J Sports Med 1997; 25:306-11
Pathology of Acute Dislocation • Hill-Sachs • Superior labral tear from anterior to posterior • Capsular tears • Rotator cuff tears • Glenoid rim fractures • Greater tuberosity fractures • Axillary nerve damage
Pathology of Acute Dislocation Repetitive Events: • Griffith et al. • Glenoid loss: • 41% in single dislocations • 86% in recurrent dislocations • Habermeyer et al. • Progressive ligamentous injury and degeneration • Sequential loss of anterior “hinges” – IGHL, labrum • Irreversible plastic deformation and degeneration occurs by the third dislocation – Point of no return
Natural History • Recurrence rates after a traumatic anterior dislocation – 14 to 97% • Consider: • Continued apprehension • Failure to return to work or sports • QOL outcome measures • Development of post traumatic arthritis
25 yr follow-up on 255 patients • 44% had no additional episodes of dislocation • 7% had only 1 recurrence • 27% had surgery for recurrent dislocation • 22% treated non-operatively for recurrent dislocation • High risk group: Age 12-22 • Recommend against immediate stabilization
Shortcomings: • Activity level not defined • DASH scores (wrist, hand) • Multiple physicians • No physical examination
131 patients, 5 yr follow-up • Age less than 25 yrs strongest predictor • Contact/collision sport athlete, overhead workers were also at a high risk of re-dislocation • Recurrence rate 33%; 43% required stabilization • ASES, WOSI scores comparable between no-op and operative groups, “copers” had lower scores • Could not recommend early surgical intervention JBJS 2007; 89:1665-74
Risk Factors for Recurrence • Age under 20 – 72-95% • Male gender • Sports activity? • Hill-Sachs Lesion • Generalized ligamentous laxity • Increased shoulder external rotation • Greater tuberosity fracture (lessens the risk)
Decision Making • Goals: • Pain-free, stable shoulder with a fully restored range of motion • Immediate goal is to reduce the shoulder dislocation
Non Surgical Management • Begins in the ER with reduction • Systematic review by Kuhn et al. • Many methods to reduce the dislocated shoulder, little data exist to identify the best method. Recommendations are based on low levels of evidence (levels 4 and 5) • Premedication with intraarticular lidocaine has fewer complications and requires a shorter time in the emergency room than intravenous sedation with no detectable differences in reduction success rates (level 1)
Non Surgical Management • Systematic review by Kuhn et al. • Post-reduction immobilization in external rotation may reduce recurrence (level 2), but immobilization in internal rotation does not (level 1). JBJS 2001; 83A:661-7
Non Surgical Management • Itoi et al. • Clinical MRI imaging shows that placing the shoulder in ER at a first time traumatic dislocation significantly improves the position of the labroligamentous lesion on the glenoid rim IR ER
Non Surgical Management • Miller et al. • 10 cadavers • Measured the contact force between the detached labrum and underlying glenoid • The contact force between the glenoid labrum and the glenoid was measured in 60° of internal rotation, neutral rotation, and 45° of • No detectable contact force was found with the arm in internal rotation • The contact force increased as the arm passed through neutral rotation and reached a maximum at 45° of ER J Shoulder Elbow Surg 2004: 13:589-92
Non Surgical Management • Itoi et al. • RCT, 198 patients immobilized in IR or ER for 3 weeks • Follow up period 2 yrs • Outcome measure: recurrent dislocation or subluxation • Lower recurrence rate in the ER (26%), IR (42%) • Greater risk reduction in the young population <30yr JBJS 2007;89:2124-31
First independent clinical assessment of the ER bracing concept by investigators other than the originators. • High-risk cohort of 51 young male patients • Follow- up: average of 33 months after the injury • Outcome: recurrent dislocation JBJS 2009 Jul;91:918-21
Recurrent dislocation occurred at a mean of 13.8 months in the external rotation group and a mean of 12.4 months in the internal rotation group • ER brace did not demonstrate a benefit in preventing recurrent dislocation compared with a standard sling • Shortcomings: • Under powered? JBJS 2009 Jul;91:918-21
Surgical Management • Historically, acute shoulder dislocation have been treated non surgically • Surgical stabilization was considered for after recurrent instability • Several studies have promoted the role of surgical stabilization after primary dislocation
Prospective randomized clinical trial • 40 patients, age <30 • Outcomes: Re-dislocation, DASH, ASES, WOSI • Immobilization for 3 weeks • Transglenoid suture repair • Both groups underwent rehabilitation Journal of Arthro Rel Res 2005: 21: 55-63
Non-surgical group – 47% recurrence rate • Surgical group -16% • WOSI was lower at 3 years in the surgical group, by 6 years not statistically significant • Recommend surgery in the young, high level athletes
Case series, average 20 year follow-up • Technique: Bioabsorbable tacks • 49 shoulders • Outcomes: Dislocation, ASES, WOSI Amer J of Sports Medicine 2009; 37: 669-673
14% dislocation rate • Excellent functional outcome scores • 14% revision surgery • Excellent subjective function and return to athletics in young, active patients with an acceptable rate of recurrence and reoperation. Amer J of Sports Medicine 2009; 37: 669-673
Cochrane Review, 2010 • Reviewed Level 1 Evidence: • Surgery significantly reduced subsequent instability • Functional assessment measures were more favorable in the surgical group • While limited, the available evidence from randomized controlled trials supports primary surgery in young adults (usually male) engaged in highly demanding physical activities who have sustained their first acute traumatic shoulder dislocation. • No guidance on the best method of surgery can be provided by this review. • There is no evidence available to determine whether surgical or non-surgical treatment is better for other categories of patient or injury.
Summary • Unrestricted function should be the measure of successful treatment not just recurrence • Discuss options with patient: • Risk factors • Anticipated activity level • Success rates of intervention selected • Individualize treatment