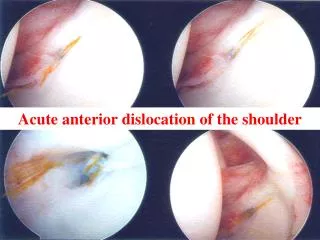
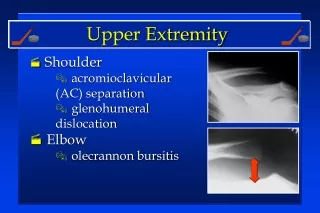
Anterior Shoulder Dislocation
Anterior Shoulder Dislocation. 17 year old basketball player Diving for basketball with arm outstretched Players landing on his posterior shoulder while he was gaining control of ball The resulting pressure from posterior resulted in subcoracoid(anterior) dislocation

Anterior Shoulder Dislocation
E N D
Presentation Transcript
Anterior Shoulder Dislocation • 17 year old basketball player • Diving for basketball with arm outstretched • Players landing on his posterior shoulder while he was gaining control of ball • The resulting pressure from posterior resulted in subcoracoid(anterior) dislocation • 90-95% are Subcoracoid(ant) or Subglenoid(ant/inf)
Didn’t see injury • Was in Training Room at time taking care of another athlete • Player presented himself to training room with arm held over stomach area • Player stated arm was numb and couldn’t move • it
The Real Issue • Player- Father in Armed Forces • Legal guardian was grandparents- not at game • Player asked that I reduce shoulder to prevent issues at home • Athletic Director was present at game- agreed
Athlete and AD relationships • Knew of the players issues at home • Very good relationship with AD • Know the family/parents when can • Don’t sit in the Training Room or the corner of the gym in isolation
Typical Protocol • Will place injured athlete in sling or ace wrap arm to side/stomach • Place ice over shirt or wrap • Send to ER for x-rays • Possible issues-- bony injuries or fractures, ligament injuries, neuro damage
What did I do • Check pulse and neuro • Palpate shoulder area- clavicle, scapula for any obvious FX • Palpate humeral head for position/ where is it at? • Check shoulders bilateral
How did I reduce? • Placed athlete prone on stomach/table • Applied 4-5 lbs of manual traction • Shoulder reduced within one minute • Subtle click or visible movement back into glenoid fossa
After Reduction • Check pulse and neuro • Palpate shoulder anatomy to check for symmetry • Placed in sling and applied ice • Sent home athletic instructions of what to look for and call me if any issues • Recheck the athlete daily basis • Asked legal guardians to call me- Never did
Follow-up care • After a few weeks we started ROM • Progressed into shoulder strengthening • Athlete ran track in spring with no complaints • Of course don’t forget to document and sit with AD to fill out paperwork
Know the athletes/AD • Speak with the kids when the come into the training room • Get on the same page with AD and know the school policies
Football Player/Dislocated Shoulder • Athlete was part of a group of players tackling ball carrier • The play ended out of bounds with about 6 players involved • Was about 20 yards away • At the end of the play one player remained on his back
Walking upon the player/injury • Player was in supine position with arm on ground outstretched and elevated- chewing on mouth piece • All UE anatomy looked to be normal
I think my arm fell off! • Was his first words • Stated his arm was numb and hoped it was still on • I reassured that it was still on
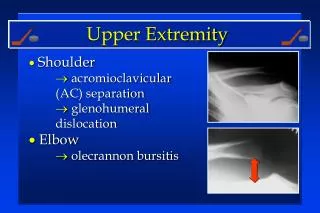
Evaluation under shoulder pads • Palpate bilateral shoulder/Cervical • Looking for Scapula FX, Clavicle FX, AC JT, Humeral Head, Cervical Spine • Check elbow, hand and wrist • Check for blood and neuro responses • Trust what you feel
Humeral Head felt like in armpit • After palpation determined dislocated shoulder
And then the wait began • Will usually rotate this back in position, resting arm on stomach and wait for parents to come down from the stands. • No parent at the game • Good relationship with AD- Policy was that players could not be transported/ambulance without parent knowledge
Stuck dislocated shoulder • Attempted to gently rotate arm into resting position on stomach • Arm would not move/ don’t force rotation • Attempted to locate parent at home– No Luck • We waited about 15 minutes with Ice on shoulder • Monitor UE vital signs
AD finally made call • Because of no obvious true emergency we waited approx 20 minutes to call Ambulance • The issue was with parents being very upset with medical bills caused by sports and not being able to pay • The AD was willing to take the responsibility of dealing with the aftermath.
Didn’t remove shoulder pads • Due to the shoulder being stuck in ext rotation and abduction/didn’t want to injury any further. • Ambulance arrived and had to transport with shoulder in that position • Get to know the AD and discuss policies so you are on the same page.
Document • Called AD re injury so we both documented
The ring finger vs logic • Football player- finger stuck in opponent players face mask • Finger will go where the opponents facemask goes • Resulting in loss of continuity between the two joints– aka- dislocated finger
Visible appearance • Usually obvious-- crooked finger, laterally or resting on top on proximal joint • Palpate carpal, metacarpal, phalanges • Once determined that FX is not an issue will reduce. Buddy tape and will play.
How to Reduce • Usually players are sweaty from participation • Gauze works well because of the rough surface, place a gauze pad over proximal, middle phalanx or metacarpal • Place a separate piece of gauze over the dislocated joint
Grasp proximal phalanx or metacarpal firmly • Grasp dislocated phalanx firmly • Lift or pull dislocated finger away from joint– Up/Down or Side • Then pull dislocated finger forward • Finger should slide into place • Check ROM, blood supply, neuro and splint
Fran VS The Ring Finger • After attempting to reduce in this manner the finger would not budge • Then I tried put more force/pull into the effort • Then I put more force/pull into the effort • Finger would not budge
Doctor VS The ring finger • Home team doc arrived upon the scene • Attempted to reduce • Then attempted to reduce again • Then attempted to reduce again • The finger Won. We had to splint in the dislocated position and send to ER with parents
The reason we lost the battle • Because of the violent twisting and pulling of the joint, soft tissue/ligament had gotten caught between the joint • Other Issues with Dislocated Fingers: • Common to have small fractures • Sometimes they when reduced they don’t stay in place. FX
Pseudoarthrosis Clavicle • Original thought to be a matchstick fracture due to pressure from birth canal.
History • Rare • Etiology Unknown—Subcalvian Artery saws through during development? • Most are occur on right side. • No hx of trauma or tenderness.
Shoulder Deformity • Normal ROM • Normal Strength • Slight Depression or forward rounding of shoulder at 9 years old. • Very mild lower scapular winging.
Treatment Options? • Surgery? • Risk of infection • Will bone graft heal/area of poor circulation • Is it worth the price? • History of surgery plate breaking • Other technique is a K wire through bone
Clavicle Pseudoarthrosis Complications • Infection • Nonunion • Brachial Plexus Injury • Rare Complications-- Pain at Site, Shoulder Asymmetry, Decreased ROM, Thoracic Outlet Syndrome.
What are we doing? • Consulting with Dr Latz • Recommend NO SURGERY