Download
1 / 61
610 likes | 1.56k Vues
Osteonecrosis in the Foot. DiGiovanni CW, Patel A, Calfee R, Nickisch F: Journal of the American Academy of Orthopaedic Surgeons 2007;4:208-217. Osteonecrosis. Avascular necrosis (AVN) Cellular death Within bone Lack of circulation Mechanical disruption of blood vessels

E N D
Osteonecrosis in the Foot DiGiovanni CW, Patel A, Calfee R, Nickisch F: Journal of the American Academy of Orthopaedic Surgeons 2007;4:208-217.
Osteonecrosis • Avascular necrosis (AVN) • Cellular death • Within bone • Lack of circulation • Mechanical disruption of blood vessels • Occlusion of blood vessels • Arterial inflow • Venous outflow
Osteonecrosis • Vascular occlusion • Trauma most common mechanical cause • Thrombosis • Embolism • Circulating fat • Abnormally shaped cells (sickle cells) • Corticosteriod use • Alcohol intake • Gaucher’s disease
Following Circulatory Compromise • Week 1-MRI negative • Few histologic changes • Week 2-MRI positive • Death of hematopoietic cell • Capillary endothelial and lipocytes seen • Lipocytes release lysosomes to acidify the tissue • Osteocytes shrink • Decrease water content of bone
Following Circulatory Compromise • Radiographic changes • Radiodensity • Bony collapse • Saponification of fat • Creeping substitution • Vacularized bone less dense than dysvascular bone
Following Circulatory Compromise • Dysvascular Bone • Collapses • Fragmentation • Sclerosis • Increases with microtrauma • Crescent sign
Following Circulatory Compromise • Bone scan • Increase uptake in early ischemic phase • Decrease uptake in later phases • SPECT • Single photon emission computed tomography • May provide better resolution
Following Circulatory Compromise • MRI • Low T1-weighted images and high T2-weighted images signal in early ischemic phase with marrow edema • Low T1-weighted images and low T2-weighted images signal in later phases
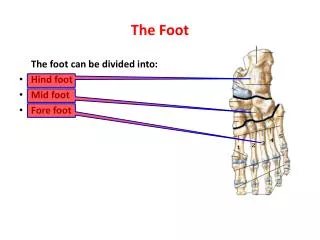
Osteonecrosis • Uncommon • Identified in almost every bone in the foot • Most common in foot • Talus • First and second metatarsals • Navicular
Osteonecrosis in the Hindfoot • Talus • Most commonly affected • At least 75% due to trauma • 25% atraumatic • No tendon or muscle attachment • Direct blood supply • Lack of vascular redundancy • >50% of bone covered with articular cartilage
Osteonecrosis in the Hindfoot • Talus • Blood Supply • Posterior Tibial artery via the artery of the tarsal canal and deltoid artery is primary blood supply • Talar body blood supply • Perforating peroneal artery and dorsal pedis artery via the artery of the tarsal sinus • Talar head and neck blood supply • Peroneal artery • Posterior process blood supply • Dorsal pedis artery • Talar head
Osteonecrosis in the Hindfoot • Talus following talar neck fracture • Hawkins Type I • Nondisplaced • 10% AVN • Hawkins Type II • Displaced with subtalar joint disruption • 40% AVN • Hawkins Type III • Displaced with ankle and subtalar incongruity • 90% AVN • Canale and Kelly Type IV • Extrusion of talar bone • Talonavicular joint subluxation • 100% AVN
Osteonecrosis in the Hindfoot • Ficat and Arlet classification of talus AVN on radiographic appearance • Stage I • Normal • Stage II • Cystic and sclerotic lesion • Normal contour of the talus • Stage III • Crescent sign • Subchondral collapse • State IV • Narrowing of the joint space • Secondary changes in the Tibia
Osteonecrosis in the Hindfoot • Talar body fracture • AVN increases with • Increased displacement • Increased comminution • Talar head fracture • High energy talar injury • AVN associated with concomitant fractures • Head • Body
Osteonecrosis in the Hindfoot • Talus atraumatic AVN etiology • Alcoholism • Sickle cell disease • Corticosteroid use • Dialysis • Hemophilia • Hyperuricemia • Lymphoma
Osteonecrosis in the Hindfoot • Talus AVN diagnosis and treatment • Symptoms within 10 months to 2 years following trauma • Rigid ORIF for fractures • Pain • Mechanical symptoms • Changes on imaging studies • Hawkins sign within 6 weeks of trauma • Late changes with incongruity of articular surface
Osteonecrosis in the Hindfoot • Talus AVN diagnosis and treatment • Non-surgical treatment • Limit weight bearing • Activity modification • Bracing and immobilization
Osteonecrosis in the Hindfoot • Talus AVN diagnosis and treatment • Surgical treatment • Arthroscopy • Core decompression • Allograft • Arthrodesis • Ankle • Subtalar • Pantalar • Vascularized bone graft • Ankle arthroplasty
Osteonecrosis in the Hindfoot • Talus AVN prognosis • Few outcome studies • Satisfactory results in less than 50% of cases
Osteonecrosis in the Midfoot • Navicular AVN • Traumatic • High energy • Most common cause of AVN • Idiopathic • Kohler’s disease • Muller-Weiss disease
Osteonecrosis in the Midfoot • Navicular blood supply • Dorsal pedis artery • Medial plantar artery • Central watershed area • Predisposes to AVN
Osteonecrosis in the Midfoot • Kohler’s disease • Childhood navicular osteonecrosis • 2-9 years old • Midfoot pain • Navicular sclerosis, fragmentation and flattening • All resolve with non-surgical management • Casting provides earlier resolution
Osteonecrosis in the Midfoot • Muller-Weiss disease • Adult onset navicular osteonecrosis • Etiology • Trauma • Delayed navicular ossification • Heel varus, pes planus, planovarus foot • Navicular sclerosis, fragmentation and flattening on radiographs • Talar head points laterally
Osteonecrosis in the Midfoot • Muller-Weiss disease • Surgical Treatment • Internal fixation of navicular • Triple arthrodesis • Talonavicular arthrodesis • Talonavicular-cuneiform bone block arthrodesis
Osteonecrosis in the Midfoot • Navicular traumatic osteonecrosis • Navicular body fractures • Type 1 • Anterior and posterior fragment • Type 2-most common • Dorsal lateral to plantar medial fracture line • Type 3 • Comminution of middle and lateral navicular • Disruption of naviculocuneiform joint
Osteonecrosis in the Midfoot • Navicular traumatic osteonecrosis • Navicular body fractures • Type 1 and 3 most commonly associated with navicular osteonecrosis • ORIF for comminuted and displaced fractures • >69% good results with ORIF
Osteonecrosis in the Forefoot • First metatarsal • Head • Idiopathic rare • Following hallux valgus correction • Post-osteotomy osteonecrosis may be up to 20% • Blood Supply • Enveloped by extensive vascular network • Dorsal pedis artery • Posterior tibial artery branches
Osteonecrosis in the Forefoot • First metatarsal osteonecrosis • Diagnosis -radiographic changes • Sclerosis • Fragmentation • Collapse
Osteonecrosis in the Forefoot • First metatarsal osteonecrosis • Treatment • Mild symptoms • Activity modification • Full length orthotic • Moderate symptoms-surgical intervention • Synovectomy • Debridement • Subchondral drilling • Salvage • 1st metatarsophalangeal arthrodesis
Osteonecrosis in the Forefoot • First metatarsal osteonecrosis • Prognosis • Postosteotomy osteonecrosis usually progress to union • Arthrodesis heals in 14 weeks
Osteonecrosis in the Forefoot • Lesser metatarsal osteonecrosis • Blood supply • 2nd through 4th metatarsal from the dorsal and plantar metatarsal arteries • 5th metatarsal has watershed area proximal
Osteonecrosis in the Forefoot • Freiberg’s disease • 2nd metatarsal subchondral collapse • Longest weight bearing metatarsal in the foot • Common in girls during adolescent growth spurt • Pain with weight bearing • Tenderness over the 2nd metatarsal head • Effusion the metatarsophalangeal joint
Osteonecrosis in the Forefoot • Freiberg’s disease • Stage I-fracture of the epiphysis • Stage II-subsidence of the central portion • Stage III-central reabsorption • Stage IV-loose body separation • Stage V-flattening, deformity, arthritis
Osteonecrosis in the Forefoot • Freiberg’s disease treatment • Non-surgical • Effective in early stages of disease • Activity modification • Limited weight bearing with crutches • Orthotics • Shoe modification • Off-load the affected metatarsal head • Limit metatarsophalangeal joint motion
Osteonecrosis in the Forefoot • Freiberg’s disease treatment • Surgical • Debridement • Loose body removal • Osteotomy • Elevation of depressed metatarsal head • Core decompression • Metatarsal head excision • Metatarsal shortening • Proximal phalanx hemiphalangectomy • Joint arthroplasty
Osteonecrosis in the Forefoot • Freiberg’s disease prognosis • Many respond to non-surgical treatment • Good results following • Partial dorsal metatarsal head resection • Synovectomy