Download
1 / 72
740 likes | 1.01k Vues
Heart Failure: Evaluation and Treatment Anecita Fadol, PhD, RN,FNP-BC Nurse Practitioner Department of Cardiology UT MD Anderson Cancer Center. Objectives. Identify the different types of cardiomyopathy Describe the pathophysiologic mechanism of cardiomyopathy/heart failure

E N D
Heart Failure: Evaluation and Treatment Anecita Fadol, PhD, RN,FNP-BC Nurse Practitioner Department of Cardiology UT MD Anderson Cancer Center
Objectives • Identify the different types of cardiomyopathy • Describe the pathophysiologic mechanism of cardiomyopathy/heart failure • Discuss diagnostic testing/procedures for heart failure diagnosis • Discuss the clinical guidelines for the management of heart failure.
Case Examples • A 16 year old male with a history of pneumonia. He was brought to the clinic by his mother because he did not seem to get better after 8 weeks since the initial flu like symptoms. Last night he had severe fatigue and shortness of breath while brushing his teeth. • A 63 year old female with a known history of breast cancer, treated with anthracycline-based chemotherapy 30 years ago. Recently, she noted progressively increasing shortness of breath with exertion, PND and lower extremity swelling.
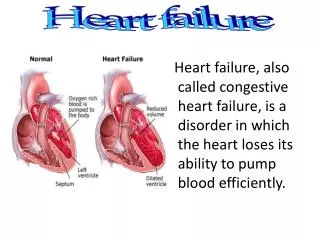
Cardiomyopathy and Heart Failure • Cardiomyopathy is a weakening or deformity of the heart muscle that causes decreased pumping force. AHA, 2008a; DeMartinis et al, 2003; Hunt et al, 2005; Yahalom et al, 2005
Risk Factors for Cardiomyopathy/HF Major causes of CMP/HF Ischemic heart disease (e.g., coronary artery disease) Nonischemic underlying diseases (e.g., hypertension, valvular heart disease) Risk factors for cardiomyopathy/HF History of or active coronary artery disease Hypertension (75% of patients) Genetic predisposition, congenital heart defects Diabetes Valvular heart disease Thyroid disease Hyperlipidemia Sleep apnea Overweight (elevated body mass index [BMI]) Sedentary lifestyle Advanced age Viral Others (e.g., smoking, alcohol, illicit or therapeutic cardiotoxic drugs) Chang, 2007; DeMartinis et al, 2003; Hunt et al, 2005
Heart Failure (HF) Definition A complex clinical syndrome in which the heart is incapable of maintaining a cardiac output adequate to accommodate metabolic requirements and the venous return.
The Donkey Analogy Ventricular dysfunction limits a patient's ability to perform the routine activities of daily living…
Epidemiology of HF in the US • 5 million symptomatic patients in 2001; estimated 10 million in 20371,2 • Incidence: about 550,000 new cases/year2 • Prevalence is 1% between the ages of 50 and 59 years3; progressively increasing to 10% over age 804 12 10 10 8 HF Patients in US (millions) 6 5 3.5 4 2 0 1991 2001 2037 1Adapted from Gilbert E. Rev Cardiovasc Med.2002;3:S42-S47. 2American Heart Association. 2004Heart and Stroke Statistical Update. 2003. 3Ho KKL et al. J Am Coll Cardiol. 1993;22:6A-13A. 4Rich M. J Am Geriatric Soc. 1997;45:968-974.
Pathological Progression of CV Disease 1 Endothelial Dysfunction CAD CM HTN Valvular Dz Arrhythmia Left ventricularinjury Low ejectionfraction Pathologicremodeling Death Pump failure Chemo Symptoms:DyspneaFatigueEdema • Neurohormonalstimulation • Endothelial dysfunction • Myocardial toxicity • Vasoconstriction • Renal sodium retention Chronicheartfailure 1 Adapted from Cohn JN. N Engl J Med. 1996;335:490–498. 2 He J, Ogden LG, Bazzano LA, et al. Risk Factors for Congestive Heart Failure in US Men and women: NHANES I epidemiologic follow-up study. Arch Intern Med 2001, 161: 996-1002.
Left Ventricular Dysfunction • Systolic: Impaired contractility/ejection • Approximately two-thirds of heart failure patients have systolic dysfunction1 • Diastolic: Impaired filling/relaxation 30% (EF > 40 %) (EF < 40%) 70% Diastolic Dysfunction Systolic Dysfunction 1 Lilly, L. Pathophysiology of Heart Disease. Second Edition p 200
Classification of HF: Comparison Between ACC/AHA HF Stage and NYHA Functional Class A At high risk for HF but without structural heart disease or symptoms of HF (eg, patients with HTN or CAD) B Structural heart disease but without symptoms of HF I Asymptomatic C Structural heart disease with prior or current symptoms of HF II Symptomatic with moderate exertion III Symptomatic with minimal exertion IV Symptomatic at rest D Refractory HF requiring specialized interventions Asymptomatic ACC/AHA HF Stage1 NYHA Functional Class2 Symptomatic 1Hunt SA et al. J Am Coll Cardiol. 2005;38:2101-2113. 2New York Heart Association/Little Brown and Company, 1964. Adapted from: Farrell MH et al. JAMA. 2002;287:890-897.
Cardiac Assessment A comprehensive cardiac assessment includes the following: Patient history Physical assessment Diagnostic testing
Cardiac Assessment: Diagnostic Testing Initial diagnostic evaluation for HF patient Echocardiogram (ECHO) Measures heart size, wall thickness/mobility, flow gradients, valvular function, LVEF Electrocardiogram Assesses cardiac rhythm, conduction; can detect myocardial infarction, arrhythmias Chest x-ray Detects heart enlargement, fluid around heart or lungs • Standard laboratory tests • Blood chemistry, urinalysis • Complete blood count (CBC) • Renal, liver, thyroid tests • Blood urea nitrogen (BUN), creatinine, albumin (liver function), glucose (diabetes) • CBC detects anemia, infection • Organ function as a contributing factor or resulting from HF Cardiac enzymes Cardiac markers Creatinine kinase (CK, CK-MB), cardiac troponins I and T Brain natriuretic peptide (BNP) • Follow-up: Assess signs and symptoms, functional capacity, body weight, understanding of treatment, compliance, exacerbating factors for HF DeMartinis et al, 2003; Chang, 2007; Fadol, 2006; Hunt et al, 2005
The Vicious Cycle of Heart Failure Management Chronic HF SOB Weight Diurese & Home Hospitalization MD’s Office IV Lasix or Admit PO Lasix Emergency Room
Goals of Heart Failure Therapy • Relieve heart failure symptoms • Improve overall clinical status • Stabilize acute episodes of decompensation • Decrease morbidity and mortality • Slow and/or reverse disease progression • Identify and treat reversible causes of LV dysfunction
General Approach to Treatment • Determine etiology and/or precipitating factors • Avoid drugs which may aggravate HF • Treat underlying disorders • Anemia, hypo/hyperthyroidism, valvular disease • Revascularization or anti-ischemic therapy in patients with CAD may reduce symptoms of HF • Physical activity (low-intensity) if stable • Restrict fluid (~2 L/day) and sodium intake (<1.5-2 g/day)
Established Therapy:Drugs with a mortalitybenefit in HF • Beta-blockers • Angiotensin converting enzyme (ACE) inhibitors • Angiotensin Receptor Blocker (Candesartan) • Spironolactone or Eplerenone • Isordil/Hydralazine
Digoxin • Mechanism of action: • contractility • Inhibition of sodium/potassium ATPase pump which acts to increase intracellular sodium-calcium exchange to increase intracellular calcium leading to increased contractility • Neurohormonal • Blunt SNS activation • Increase vagal tone • Slow conduction, prolong AV refractoriness, slowing ventricular response in atrial fibrillation
Pharmacologic Management Digoxin • Enhances inotropy of cardiac muscle • Reduces activation of SNS and RAAS • Controlled trials have shown long-term digoxin therapy: • Reduces symptoms • Increases exercise tolerance • Improves hemodynamics • Decreases risk of HF progression • Reduces hospitalization rates for decompensated HF • Does not improve survival
Digoxin • Warnings/Precautions • Acute myocardial infarction • Acute myocarditis or amyloid cardiomyopathy • Correct electrolyte imbalances • Adjust dose in renal disease • Bradycardia • Withdrawal in CHF patients may lead to recurrent CHF symptoms • Drug interactions • Digoxin toxicity
Digitalis Compounds Like the carrot placed in front of the donkey
Pharmacologic Management Diuretics • Used to relieve fluid retention • Improve exercise tolerance • Facilitate the use of other drugs indicated for heart failure • Patients can be taught to adjust their diuretic dose based on changes in body weight • Electrolyte depletion a frequent complication • Should never be used alone to treat heart failure • Higher doses of diuretics are associated with increased mortality
Diuretics • Diuretics and salt restriction are indicated in patients with current or prior symptoms of HF and reduced LVEF who have evidence of fluid retention (Class I; LOE C) • Use until euvolemic stage is achieved • Continue to prevent recurrence of fluid retention • Increase urinary sodium excretion • Improve pulmonary and peripheral congestion • Decrease preload • No long-term studies • Effects on morbidity and mortality are unknown ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
Dosing Oral Diuretics ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
Dosing IV Diuretics ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
ACE inhibitors • Mechanism of action: • preload and afterload • Arterial and venous dilatation • Reduces formation of Angiotension II (vasoconstrictor) • Reduces breakdown of bradykinin (vasodilator) • Clinical Effects: • Improve symptoms • Reduce remodeling / progression • Reduce hospitalization • Improve survival
Ace Inhibitors • Recommendations • ACEIs are recommended for all patients with current or prior symptoms of HF and reduced LVEF , unless contraindicated (Class I; LOE A) • ACEIs should be used in all patients with reduced LVEF and no symptoms of HF, even if they have not experienced MI (Class I; LOE A) • ACEIs or ARBs can be beneficial in patients with HTN and LVH and no symptoms of HF (Class IIa; LOE B) ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
Effect of ACE Inhibitors on Survivalin Heart Failure P=0.30 P<0.0036 P<0.003 Placebo Enalapril Placebo Mortality From All Causes (%) Cumulative Mortality Cumulative Predictability of Death Enalapril Enalapril Hydralazine Isosorbide Dinitrate Months Months Months SOLVD-PSOLVD-T CONSENSUS NYHA Class Class I-II (N=4228) Class II-III (N=2569) Class IV (N=253) Treatment Enalapril Enalapril Enalapril Results 8% 16% 27% (% reduction in all-cause mortality) 1The SOLVD Investigators. N Engl J Med. 1991;325:293-302. 2Cohn J et al. N Engl J Med. 1991;325:303-310. 3The CONSENSUS Trial Study Group. N Engl J Med. 1987;316;1429-1435.
ACE inhibitors ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
Contraindications: Hypersensitivity Angioedema related to previous treatment with ACEI Hereditary angioedema Bilateral renal artery stenosis Pregnancy (2nd and 3rd trimester) Warnings/Precautions: Anaphylactic reactions can occur Angioedema can occur at any time during treatment, especially after 1st dose Careful BP monitoring with 1st dose (hypotension) Captopril>Lisinopril>Enalapril May cause hyperkalemia, rise in Scr Ace Inhibitors
Principles of ACEI therapy • Occurrence of ARF should prompt a search for: • Hypotension (MAP <65 mmHg), volume depletion, or nephrotoxin administration • Correct or remove these factors • Consider bilateral renal artery stenosis • ACEIs should be discontinued temporarily while precipitating factors for ARF are corrected • ARBs are not an appropriate substitute under these conditions!!! • ACEI therapy can be reinstituted once these factors are corrected • Hyperkalemia is a potential complication, particularly in patients with DM or CRF • Monitor K+ early after initiation of therapy, reduce dietary K+, avoid agents that aggravate hyperkalemia
ACE inhibitors • Start with a low dose • Increase dose if well tolerated (hold parameters for BP and HR) • Dose NOT determined by symptoms, titrate to target dose • Monitor renal function & serum K+ • Avoid initiating while volume depleted
Diuretics, ACE Inhibitors Reduce the number of sacks on the wagon
ARBs • Recommendations • ARBs approved for the treatment of HF are recommended in patients with current or prior symptoms of HF and reduced LVEF who are ACEI intolerant(Class I; LOE A) • ARBs are reasonable to use as alternatives to ACEIs as 1st line therapy for patients with mild to moderate H F and reduced LVEF, especially for patients already taking ARBs for other indications (Class IIa; LOE A) • The addition of an ARB may be considered in persistently symptomatic patients with reduced LVEF who have already been treated with conventional therapy (Class IIb; LOE B) ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
ARBs ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
Beta-blockers • Recommendations • Beta-blockers and ACEIs should be used in all patients with recent or remote history of MI regardless of EF or presence of HF (Class I: LOE A) • Beta-blockers are indicated in all patients without a history of MI who have reduced LVEF with no HF symptoms(Class I: LOE C) ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
Pharmacologic Management Beta-Blockers • Cardioprotective effects due to blockade of excessive SNS stimulation • In the short-term, beta blocker decreases myocardial contractility; increase in EF after 1-3 months of use • Long-term, placebo-controlled trials have shown symptomatic improvement in patients treated with certain beta-blockers1 • When combined with conventional HF therapy, beta-blockers reduce the combined risk of morbidity and mortality, or disease progression1 1 Hunt, SA, et al ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult, 2001 p. 20.
Beta-blockers • Mechanism of action: • Density of ß1 receptors • Neurohormonalactivation • Slow/reverse ventricular remodeling • Decreased myocyte death from catecholamine- induced necrosis or apoptosis • HR • Symptomatic worsening of HF • Low doses, slow upward titration • Antiischemic • Antihypertensive • Antiarrhythmic • Antioxidant, Antiproliferatiev
Beta-blockers • Increase EF • Decrease ventricular mass • Reduce systolic and diastolic volumes • Decrease hospitalization and mortality • Greater benefit seen at higher doses
Even low doses of B-blockade can have a dramatic effect Ejection Fraction* ‡ 8 P<.001 † 6 † LVEF (EF units) 4 2 0 Placebo 6.25 mg bid 12.5 mg bid 25 mg bid Carvedilol Patients receiving diuretics, ACE inhibitors, ± digoxin; follow-up 6 months; placebo (n=84), carvedilol (n=261). *Results from the Multicenter Oral Carvedilol Heart Failure Assessment (MOCHA) trial (n=345). †P.005 vs placebo. ‡P.0001 vs placebo. Adapted from Bristow MR et al. Circulation. 1996;94:2807–2816.
Effects of Beta-Blockers on Mortality -blocker -blocker -blocker b b b P <0.0001 1.0 1.0 1.0 Placebo Placebo Placebo 0.8 0.8 0.8 Mortality Risk • 34 % Risk Risk • 35 % 34 % ¯ 0.6 0.6 0.6 P=0.006 P<0.00013 0 1 2 Time (years) 0 1 2 0 1 2 CIBIS II MERIT-HF COPERNICUS NYHA Class III-IV (N=2647) II - IV (N=3391) IV (N=2289) Entry criteria LVEF 35% LVEF 40% LVEF 25% Treatment Bisoprolol Metoprolol CR/XL Carvedilol Results 34%34%35% (% reduction in death) 1. CIBIS II Investigators and Committees. Lancet. 1999;353:9-13. 2. MERIT-HF Study Group. Lancet. 1999;353:2001-2007. 3. Packer M et al. N Engl J Med. 2001;344:1651-1658.
Beta-blockers • Recommendations • Beta-blockers and ACEIs should be used in all patients with recent or remote history of MI regardless of EF or presence of HF (Class I: LOE A) • Beta-blockers are indicated in all patients without a history of MI who have reduced LVEF with no HF symptoms(Class I: LOE C) ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult http://www.acc.org/clinical/guidelines/failure/hf_index.htm
ß-Blockers Limit the donkey’s speed, thus saving energy
Beta-blockers Contraindications: • Cardiogenic shock, symptomatic hypotension • Hypersensitivity • Bradycardia HR<45 • 2nd and 3rd degree heart block; (P-R interval greater than or equal to 0.24 sec) – unless pacemaker places
Beta-blockers Warnings/Precautions: • Anesthesia/surgery (myocardial depression) • Bronchospastic disease (less with cardioselective agents) • Decompensated HF • May mask s/sx hypoglycemia • May mask signs of hyperthyroidism/thyrotoxicosis • PVD – use with caution since may aggravate arterial insufficiency • Avoid abrupt withdrawal (may result in hypertension, tachycardia, ischemia, angina, MI, and sudden death) – discontinue over 1-2 weeks