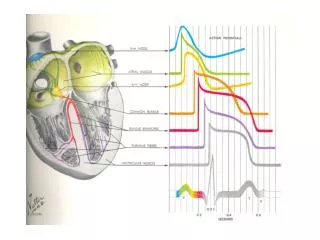
Narrow Complex Tachycardias
830 likes | 2.41k Vues
Narrow Complex Tachycardias. Moritz Haager PGY-5. Objectives. Develop an approach Review treatment options Dispositon decisions. Perspective. SVT Broad umbrella term for any tachycardia originating above the ventricles Variable underlying mechanisms but basically one Tx approach

Narrow Complex Tachycardias
E N D
Presentation Transcript
Narrow Complex Tachycardias Moritz Haager PGY-5
Objectives • Develop an approach • Review treatment options • Dispositon decisions
Perspective • SVT • Broad umbrella term for any tachycardia originating above the ventricles • Variable underlying mechanisms but basically one Tx approach • Ranges from physiological pathological, and benign dangerous • Occurs in all age groups • Clinical presentation from asymptomatic shock / CHF When presented with an undifferentiated presentation with a broad DDx and variability in outcome you need an APPROACH
Why should we care? • Morbidity & Mortality • Patient discomfort & anxiety • Syncopal events (falls) ~15% • Risk of sudden cardiac death w/ accessory pathway driven arrhythmias • Tachycardia-mediated cardiomyopathy • LV dilatation w/ impaired LV function
Approach to Tachycardia • Stable or unstable? • Assess ABC’s, O2, IV, monitors, crash cart to bedside • In general if unstable, give’m juice • Narrow or wide QRS? • Regular or irregular? • Look at the P waves • Relationship to QRS • P wave axis / rate • P wave morphology(ies) • What is the trigger / underlying cause?
Step 1: Stable or Unstable? • Not always black & white • Continuum from stable compensated decompensated shock arrest • Stability determined by big picture: • Symptoms, signs, & vitals • Cardio-respiratory reserve • Age • Co-morbidities • Be prepared • Any dysrhythmia could potentially deteriorate • All therapies are potentially pro-arrhythmic
Step 2: Narrow or wide? • Measure widest QRS on ECG • Adults: wide = >0.12 sec (3 small boxes) • Kids <8yo: wide = >0.08 sec (2 boxes)
Step 3: Regular or Irregular? • Use calipers or paper • Irregularity can be subtle, esp at fast rates • Generally • Irregular rhythms originate ABOVE the AV node • VT is almost never irregular
Step 4: Look at the P waves • P waves present? • Is there a P before every QRS? • What is the relationship b/w the P and the QRS? • What is the P wave rate? Ventricular rate? • Is the P wave coming from the SA? • N axis: upright in II, negative in aVR • Is there >1 distinct P wave morhology?
Diagnostic Trick: 50 mm/s ECG Tracings • Comparsion study of 8 EP’s • Given 45 ECG’s of NCT’s printed at 25 mm/s & asked to give Dx & Tx plan • 2 wks later given same ECG’s printed at 25 & 50 mm/s & asked to give Dx & Tx • Results • 50 mm/s increased diagnostic accuracy from 63 to 71%, P=0.002 • J Emerg Med 2002; 22: 123–126
Final Categorization • Narrow Complex Tachycardias • Regular w/ P’s • = sinus, a. flutter w/ constant block, Focal atrial tachycardia, AVNRT, junctional tachycardia • Irregular w/ P’s • = MAT, a. flutter variable block • Regular, no P’s • = AVRT, AVNRT • Irregular, no P’s • = a. fib • Wide Complex Tachycardias Tx w/ AV nodal blockers Rate control +/- rhythm control
Step 5: Underlying Causes • HIS DEBTS • H – Hypoxia • I – Ischemia / infarction • S – Sympathetic excess • Hyperthyroid, CHF, pheochromocytoma, excercise • D – Drugs • Anti-arrhythmics, cocaine, amphetamines, caffeine, etc • E – Electrolytes • K+, Ca2+, Mg2+ • B – Bradycardias • Eg. Sick sinus syndrome • T – Thyroid disease • S – Stretch • Hypertrophy / dilation of atria & ventricles (CHF, valvular Dz) Preciptants vary w/ age, sex, co-morbidities, etc
Clinical Presentations • Typical Sx • Palpitations 96% • “Dizziness” 75% • Dyspnea 47% • Fatigue 23% • Chest pain 35% • Diaphoresis 17% • Nausea 13% • Neck pounding said to be pathogonomonic
Case • 27 yo M w/ palpitations & dyspnea • NCT at 160 on ECG c/w PSVT • Also tells you he has been “pissin’ like a racehorse” • Does he have diabetes?
Polyuria in PSVT • Loss of AV synchronization • Atrial contraction against closed AV valves • Elevated atrial pressure & atrial stretch • Release of atrial natriuretic peptide polyuria NB: This is trivia – absence of polyuria does NOT exclude Dx of PSVT and you should still check at least a urine for glucose
Case • 3 mo F w/ dyspnea & wheeze • T 40.5oC, P 190, RR 60, SpO2 88% • Mod resp distress on exam w/ wheezes & crackles bilaterally • Is this just sinus tachycardia from her fever?
Tachycardia & Fever • Prospective observational study of 490 infants <1 yo • Measured HR & rectal temp in calm, quiet kids w/o evidence of serious illness • Analyzed relationship b/w HR & temp w/ multivariate linear regression • Results • HR increased ~10 bpm for every 1oC rise in infants b/w 2 -12 mo • Ann Emerg Med. 2004;43:699-705
Tachycardias: Mechanism • Reentry • 50-80% of NCT’s • Abrupt on-/off-set • Do well w/ electricity • Enhanced automaticity • Typically catecholamines, drugs, lytes, ischemia • Gradual on-/off-set • Not likely to respond to electricity; Tx underlying cause • Triggered dysthythmias • Interruption of repolarization by afterdepolarizations • Ischemia, drugs, lytes, catecholamines • Not likely to respond to electricity; Tx underlying cause E.g. Torsades IV magnesium
Maximal sinus tach • 220 – age = maximum HR • 220 -80 = 140 • Unlikey this is just sinus tach
Regular NCT: DDx • P waves present: • Sinus tachycardia • Atrial Flutter • AVNRT • AVRT • Focal Atrial Tachycardia • No P-waves • AVRT • AVNRT • Junctional Tachycardia Consider under PSVT as can be impossible to differentiate on ECG; Tx generally the same
AV nodal reentrant tachycardia Most common PSVT (>60%) Dual AV nodal physiology 2 separate conduction paths in AV node Fast pathway Slow pathway Allow for re-entry circuit w/in AV node Atrioventricular reentrant tachycardia accessory pathway(s) (AP) = Tracks of conducting tissue outside of AV node, connecting atria & ventricles Re-entry circuit formed by AP & AV node (WPW) 2 or more separate AP’s (bypass AV node completely) AVNRT vs. AVRT
AVNRT • “Typical” AVNRT – = 90-95% • Anterograde conduction down slow pathway • Retrograde conduction up fast pathway • If P waves seen RP < PR interval ATRIA VENTRICLES “Atypical” AVNRT is the reverse of what is pictured here
2 types of AP “concealed” = capable of retrograde conduction only “manifest” = allow anterograde +/- retrograde conduction See “pre-excitation” on ECG AVRT
WPW (Wolf-Parkinson-White) PR <120 msec QRS >100 msec Delta waves in some leads LGL (Lown-Ganong-Levine) PR <120 msec Preexcitation Syndromes
Orthodromic SVT Anterograde via AV & returns via accessory tract Uses normal conduction system therefore get narrow complex tachycardia WPW & SVT Orthodromic makes up 90-95% of WPW SVT’s
WPW & SVT • Antidromic SVT • Anterograde conduction from atria to ventricles via accessory path & retrograde flow through AV node • Wide complex tachycardia • Avoid AV nodal blockers • Use procainamide or cardiovert (5-10% of WPW SVT)
WPW & A Fib • IrregularWide complex tachycardia • May see capture & fusion beats • Common (~30% of WPW pts) & potentially life-threatening • AP w/ short refractory period & anterograde conduction near 1:1 conduction VF • 0.15 – 0.39% incidence of sudden cardiac death • Do NOT block AV node • Channels all impulses down AP & increases risk of VF • Use Procainamide or cardioversion
Predictors of Sudden Cardiac Death in WPW • Shortest pre-excited R-R interval during atrial fib <250 ms • Hx of symptomatic tachycardia • Multiple accessory pathways • Ebstein’s anomaly* • Blomström-Lundqvist et al. ACC/AHA/ESC Guidelines for Management of SVA ACC 2003; 42:1493–531 *= abnormal tricuspid valve regurgitation & RA enlargement
AVNRT vs. AVRT: Can you tell them apart • Helpful ECG findings • Pseudo R’ in V1 • Pseudo S in II, III, aVF • specific (but not sensitive) for AVNRT • ST elevation in aVR • RP >100 ms • ST depression ≥2mm • Suggest (not highly specific or sensitive) AVRT Bottom line = 12-lead lacks 100% accuracy but important to look because AVRT more serious Dx See Adam Osters talk July 22, 2004 for more detailed explanation
PSVT: Acute Treatment Summary • Unstable • DC cardioversion • Stable • 1) Vagal maneuvers (Class I/ level A) • 2) Adenosine (Class I/ level A) • 3) CCB’s (Class I/ level A) • 4) BB’s (Class IIb/ level C) • 5) Amiodarone (Class IIb/ level C) • 6) Digoxin (Class IIb/ level C) Blomström-Lundqvist et al. ACC/AHA/ESC Guidelines for Management of SVA JACC 2003; 42:1493–531
Cardioversion • Sedation • ?1 mg midaz + 100 mcg fentanyl • Energy Levels • PSVT:- 50 Joules • Atrial fibrillation: 200 Joules • Atrial flutter: 25-50 Joules • Orthodromic WPW: 50 Joules • Narrow Complex VT: 50-100 Joules
Adenosine • Actions • Coronary vasodilator • Transient SA & AV nodal blockade • Outward K+ current hyperpolarizes cells • Reflex catecholamine release & sympathetic discharge • T1/2 <10 sec; • Duration of action 30-40 sec
Adenosine: Adverse Effects • Hot flash / flushing ~25% • Dizziness ~20-50% • Chest pain / pressure ~20-40% • Dyspnea ~10-25% • Feeling of impending doom ~10% • Pro-arrhythmia / blocks ~10% >75% of pts will experience side effects w/ adenosine
Adenosine: Pro-arrhythmic Effects • Significant literature reports • A fib, VF, Transient sinus arrest / asystole, Torsades de pointes • Prospective observational ED study • 160 consecutive pts given adenosine • Overall 21 (13%) pts had pro-arrhythmic s/e • Prolonged AV block (>4sec) 11 (7%) • Atrial Fib 2 (1%) • Non-sustained VT 8 (5%) • All resolved spontaneously; no serious outcomes Euro J Emerg Med 2001; 8: 99-105
Pearls • Adenosine CAN convert some VT, • giving it to “diagnose” SVT w/ aberrancy is misguided • Wide & irregular – think WPW + A fib • NO AV nodal blockers • Amiodarone may not be ideal • Procainamide is the drug of choice
Adenosine: Drug Interactions • Theophylline • ↑’s dose requirement • Dipyridamole • ↓’s dose requirement • Carbamazepine • potentiates adenosine-induced heart block • CCB’s / BB’s • Potentiate hypotension & bradycardia
Adenosine Dosing • DBRCT of 201 pts w/ PSVT: • Adenosine Dose Conversion Rate • 3 mg 35.2% • 6 mg 62.3% • 9 mg 80.2% • 12 mg 91.4% • P<0.001 for all doses c/w placebo • All administered through PIV DiMarco et al. Ann Intern Med 1990; 113: 104-110
Practical Pearl • Adenosine administration • Want to get it in as fast as possible • Use 2 syringes w/ 18g needles • one w/ adenosine • Other w/ 10 cc NS • Put both needles into IV access port • Push the adenosine w/ one hand and… • …chase immediately w/ the NS w/ the other • NB: want an IV in the AC if at all possible
Adenosine via Central Line • Appears to have increased success rate • Observational study of 200 pts w/ PSVT induced in EP lab • found 99% success rate w/ 12 mg via femoral line • Strickberger et al. Ann Intern Med 1997; 127: 417-422 • Randomized Cross-over study of 30 pts given adenosine via PIV or central line • success rate w/ 3 mg was 77% when given via central line vs. 37% via PIV • McIntosh-Yellin et al. JACC 1993; 22:741–5 • Case reports of more severe S/E via central line (felt to be dose-related)
Case 4 • 31 yo F w/ PSVT • Vagal maneuvers fail • 6 mg adenosine IV no response • 12 mg adenosine IV slows down briefly • What now? Would you give her 18 mg of adenosine?
High Dose Adenosine • Background • ACLS: 6 mg, then 12 mg x2 if unsuccessful • FDA approves use up to 12 mg • Literature reports of uses up to 25 mg • What about higher doses? • Randomized cross-over comparison of of 31 pts w/ AVNRT/AVRT in EP lab given 12 & 18 mg adenosine via PIV • Non-significant increase in efficacy w/ 18 mg • 25/31 (81%) vs. 29/31 (94%); P = 0.103) • No significant increase in adverse effects • may have been underpowered to find difference Weismueller et al. Deutsche Med Wochenschrift 2000. 125: 961-69
Calcium Channel Blockers • 2nd line agents in PSVT • Verapamil • 1st dose: 2.5 – 5 mg IV over 2 min • 2nd dose (30 min later): 2.5 – 10 mg IV over 2 min (to max of 20 mg) • NB: CONTRAINDICATED in <1yo (risk of EMD), wide QRS, or hypotensive pts, CHF, or WPW • Diltiazem • 1st dose: 0.25 mg/kg IV over 2 min • 2nd dose (15 min later): 0.35 mg/kg IV over 2 min followed by gtt of 5-15 mg/h • Generally felt to be safer than Verapamil but same cautions apply
What about Verapamil? • RCT of 122 pts w/ PSVT treated w/ either adenosine or Verapamil • NS difference in conversion to NSR • 86.0% (52/60) vs. 87.1% (54/62), p=NS • Adenosine worked much faster • 34.2 +/- 19.5 sec vs. 414.4 +/- 191.2 sec, P < 0.0001 • Cheng KA Zhonghua Nei Ke Za Zhi 2003; 42(11): 773-6
Adenosine vs Verapamil DBRCT of 70 pts w/ PSVT DiMarco et al. Ann Intern Med 1990; 113: 104-110
Retrospective study of 106 pts w/ PSVT treated w/ adenosine or verapamil No sig difference in overall efficacy Logistic regression found Adenosine worked better w/ faster HR Verapamil had better success w/ slower HR Adenosine vs. Verapamil Interesting study, but hypothesis-generating at most; needs prospective, randomized investigation Euro Heart J 2004; 25: 1310–1317
Case • 78 yo F presents w/ NCT • Hx of PSVT – ECG looks identical • Had severe side effects w/ adenosine previously & refuses repeat • Does not want to be shocked either • When you ask for Verapamil the nurse points out her pressure is only 88/65 • What can you do?
Calcium pre-Tx to prevent CCB-induced hypotension • Verapamil = vasodilator + myocardial depressant • Get some decrease in BP (5-40 mm Hg) in up to 75% pts when given via IV route • No RCT’s looking at Ca2+ pre-Tx • 6 trials totalling 322 pts suggest pre-Tx blunts Verapamil-induced decrease in BP • Ca gluconate 1g IV over 5 min appears to be a reasonable choice • Ann Pharmacother 2000; 34: 622-9. NB: No studies exist on Ca2+ pre-Tx for IV Diltiazem
PSVT: Chronic Tx • Pts w/ frequent episodes / severe Sx • Drugs • CCB’s • B-blockers • Digoxin • Other antirhythmics • Pill-in-pocket approach • Dilitiazem 120 mg PO + propranolol 80 mg PO appears to work best • Rarely get hypotension or bradycardia • Decreases ED visits • Catheter ablation techniques in EP lab • Curative in >90% of pts – becoming 1st line May be reasonable to start in ED, but need reliable F/U Better left to cardiology or EP