Understanding Cumulative Trauma
Understanding Cumulative Trauma. TM 655 Carter J. Kerk SDSMT Summer 2008. Assignment. Read MacLeod, Chapter Three Read Gabriel, Chapter Three Do Case Example 3 (CE3) At least 2 pages of double-spaced text What were your impressions? What surprised you?

Understanding Cumulative Trauma
E N D
Presentation Transcript
Understanding Cumulative Trauma TM 655 Carter J. Kerk SDSMT Summer 2008
Assignment • Read MacLeod, Chapter Three • Read Gabriel, Chapter Three • Do Case Example 3 (CE3) • At least 2 pages of double-spaced text • What were your impressions? • What surprised you? • Submit on email with proper subject line
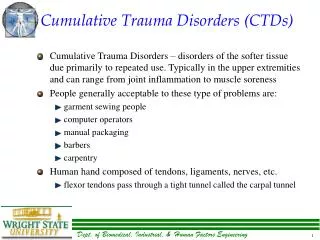
What is cumulative trauma? • Wear and tear on joints and surrounding tissues over time because of overuse • Cumulative vs. Acute • Low Back • Cervical Spine (neck) • Upper Extremities • Shoulder, elbow, wrist, fingers
Musculoskeletal & Neurovascular Disorders • Disorders of muscles, joints, tendons, ligaments, nerves, cartilage • usually a gradual buildup of stress to the musculoskeletal system and neurovascular system • diagnosis by a qualified medical expert • most common in upper extremities and spine
Disorder Terminology • Cumulative Trauma Disorders (CTDs) • Repeated Motion Disorders (RMIs) • Repetitive Strain Injuries (RSIs) • Musculoskeletal Disorders (MSDs) • Involving muscles and connective tissue • Connective Tissue (bone, cartilage, tendon, ligament, fascia) • Neurovascular Disorders (NVDs) • Involving nerves and blood vessels
MSD / NVD Symptoms • Vague, Slow to Develop • Soreness, pain, discomfort • Numbness, tingling sensations • Weakness, clumsiness • Burning sensations • Limited range of motion • Joint stiffness, popping/cracking in joints
Diagnosis • Difficult to diagnose • Proper diagnosis should only be done by a qualified medical professional • Certified Occupational Physician (Occ Doc) • By training, experience, examination in occupational illness/disease • A few specialists • Not most doctors, any nurses, ergonomist, physical therapists, occupational therapists, engineers, managers, etc.
Treatment • Ice • Anti-inflammatory drugs • Rest • Possibly cortisone • Physical therapy (strengthening, stretching, work hardening, etc.) • Surgery (only as a last resort) • “Job Re-Design”
Early Recognition • Early recognition is important in controlling MSDs / NVDs • Use early warning systems (e.g. body discomfort surveys) • Training of employees and managers • Working relationship with Occ Doc • Stress “conservative treatment” • Non-surgical
The Risk Factor Model Lack of Rest Work/Rest Ratio Shift Length Environment Sustained Repetition Occupational Vibration Non-Occupational Temperature Posture Physical & Temporal Risk Factors Force Personal Psychosocial Compounding Risk Factors
Wrist Disorder Rates by Exertion & Repetition (n=574, Silverstein, 1985)
MSDs / NVDs Categorized by Body Part • Hand and Wrist • Elbow and Shoulder • Back, Neck, and Torso • Legs
Wrist • Bones • Ligaments • Tendons • Nerves • Carpal Tunnel
Elbow • Bones • Humerus (medial & lateral epicondyle); radius, ulna. • Muscles • Forearm muscles attach at elbow. • Nerves • Ulnar nerve.
THE SHOULDER Anatomy • Bones • Muscles • Ligaments • Bursa • Cartilage
Hand and Wrist Disorders • Carpal Tunnel Syndrome (CTS), Tendonitis, De Quervain’s Disease, Digital Neuritis, Ganglion Cyst, Guyon Tunnel Syndrome, Synovitis, Trigger Finger
Elbow and Shoulder Disorders • Bursitis, Epicondylitis, Radial Tunnel Syndrome, Rotator Cuff Tendonitis, Thoracic Outlet Syndrome
Back, Neck, and Torso • Degenerative Disc Disease, Herniated Disc, Ligament Sprain, Mechanical Back Syndrome, Muscle Strain, Posture Strain, Tension Neck Syndrome, Hernia
Legs • Patellar Synovitis, Phlebitis, Plantar Fascitis, Shin Splints, Sub-Patellar Bursitis, Trochanteric Bursitis
Categories of Upper Extremity CTDs • Tendon disorders • Nerve disorders • Neurovascular disorders
Tendon Disorders • Tendonitis • tenosynovitis • De Quervain’s disease • stenosing tenosynovitis crepitans (trigger finger) • ganglionic cyst • lateral epicondylitis (tennis elbow) • medial epicondylitis (golfer’s elbow) • rotator cuff tendonitis
Nerve Disorders • Cubital tunnel syndrome • Carpal tunnel syndrome (CTS)
Neurovascular Disorders • Thoracic outlet syndrome • Vibration syndrome • white finger or Raynaud’s phenomenon
Swelling of tendons. Decreased blood supply to median nerve. Numbness/tingling in fingers. Prolonged irritation – scarring & nerve damage. Repetitive or strenuous activity. Carpal Tunnel Syndrome
DeQuervain’s Tenosynovitis • Swelling of tendon sheath that surrounds thumb tendons as they travel through the wrist to the thumb. • Overuse. • Strain injury. • Inflammatory arthritis.
Trigger Finger • Tendon thickens and bends finger. • Arthritis, diabetes, lacerations, infections. • Repeated “pistol gripping” of power tools. • Long hours grasping steering wheel.
Lateral Epicondylitis • Tennis Elbow • Chronic tendinosis of the wrist and finger extensors at their insertion at the elbow. • Tendons of forearm become irritated or tear away from medial or lateral epicondyle causing irritation. • Overuse of forearm muscles used for rotation of the arm and extension of wrist.
Medial Epicondylitis • aka. Golfer’s Elbow • Overuse of the flexor-pronator muscles whose origin is at anterior medial epicondyle of humerus • Sports related • Occupation related • Screwdriver, hammer use
Ulnar nerve entrapment • Muscle, ligament, & bone make up cubital tunnel. • Ulnar nerve travels medially. • Frequent elbow bending – pulling levers, reaching, lifting. • Repeated injury or pressure. • Resting elbow on hard surface for long periods. • Direct blow or injury to ulnar nerve. • Anatomy- nerve shifts, snaps over bone irritation.
Rotator Cuff Injuries. • Single traumatic injury. • Collisions, fall on an outstretched hand • Multiple “micro-traumas” over time. • Repeated overhead activity. • Heavy lifting. • Normal degeneration in 3rd and 4th decades of life. • Most commonly the supraspinatus.
Impingment: Rotator Cuff Tendonitis or Shoulder Bursitis • Tendons become red, sore, & inflamed usually from crowding by surrounding structures. • Trapped under acromium(impingement) • Inflammation of the bursa usually occurs too. Causes – Overuse (frequent overhead reaching); Rheumatoid arthritis.
Low Back Pain (LBP) Categories • Muscular / Ligamentous • strain • Structural • overloading trauma, degenerative disease, facet dysfunction, osteoporosis, scoliosis • Discogenic • herniation, nerve irritation, tumor • Others • infections, congenital disorders
? Magnitude and Trend: Numbers and types of occupational illness cases between 1972 and 2001. (DHHS 2004, Fig 1-22)
What are the reasons for the dramatic increase thru mid 90s? • Aren’t these the same jobs workers have been doing for decades? • Are workers getting weaker or wimpier? • Increased awareness and reporting? • Technological changes? • Aging workforce?
Increase in Awareness & Reporting • MSDs have probably existed since the Stone Age • Only recently have we begun recording • Increased media exposure • Proactive training • Work expectations (we may no longer be willing to accept the pain) • Employees realize they can receive compensation (for suffering or faking)
Increase in Awareness & Reporting (continued) • Diagnostic techniques have improved • Easier access to medical care and treatment • Companies are required by OSHA to record work-related disorders • When you start a new program, be prepared for a spike in reporting the first few years • Increased consciousness
Changes in Technology • Increase Specialization of Tasks • Typewriters to keyboard • Drafting tables to CAD software • Chicken at the grocery store • Increases in Assembly Line Work • Traditionally started in the automotive industry, now common in many sectors • Gaps in Automation • Highly automated processes may be interspersed with repetitive human tasks
Fads and Malingerers? • Fad? • “Australian Disease” (see course website) • Reporting phenomenon, increase attention in media • Ergonomics and CTDs are no fad! • Malingerers? • There is a problem – Workers’ Compensation • Malingerers are not the primary cause of increased claims
? Magnitude and Trend: Numbers and types of occupational illness cases between 1972 and 2001. (DHHS 2004, Fig 1-22)
What are the reasons for the gentle decline since mid 90s? • Effects of ergonomics programs? • Effects of medical management? • Better overall understanding of the problem?
Were MSDs invented in the 1980s? • MSDs are Age-Old • Read cases on p. 76-78 • MSDs in the 1700s • MSDs in Literature
![Cumulative distribution [%]](https://cdn1.slideserve.com/2142714/slide1-dt.jpg)