Download
1 / 24
240 likes | 267 Vues
The SHARE initiative led by Peter Langhorne at the University of Glasgow focuses on the assessment, management, and evaluation of hyperacute stroke cases in Scotland. With over 10,000 new strokes annually and 70,000 Scots living with stroke consequences, this program aims to improve outcomes and reduce costs through timely interventions. The project has driven up standards, particularly in thrombolysis for acute strokes, emphasizing that time is crucial in achieving better recovery rates. Various inclusion criteria help identify eligible patients for thrombolytic treatment, while exclusion criteria ensure patient safety and optimize outcomes. The initiative stresses the importance of specialized stroke units, trained staff, immediate imaging access, and teleconsultation for swift decision-making. Through data collection and analysis, the project aims to refine stroke care protocols and enhance patient outcomes.

E N D
Scottish Hyperacute stroke Activity Register and Evaluation (SHARE) Peter Langhorne University of Glasgow
What’s in a name? S – Scottish H - Hyperacute A – Assessment and M - Management E - Evaluation
What’s in a name? S – Scottish H - Hyperacute I - Investigation and T - Treatment E - Evaluation
What’s in a name? S – Scottish H – Hyperacute stroke A – Activity R – Register and E - Evaluation
Stroke in Scotland • Over 10,000 people have a new stroke each year • 70,000 Scots living with consequences of a stroke • Average lifetime cost of stroke £45,000 • Good progress in developing services • SSCA has help drive up standards
Thrombolysis in acute stroke Before After
In 2002, European Union regulatory authority approved rt-PA for stroke CONDITIONALLY • Within 3 hours of an ischaemic stroke • Age 18-80 • In high quality stroke centres with stroke units with certain monitoring requirements
Time is Brain Impact of thrombolysis Number making full recovery per 100 treated 30 20 10 0 Benefit 0 2 4 6 Time (hours) Saver, Stroke 2006
Time is Brain Impact of thrombolysis Number making full recovery per 100 treated 30 20 10 0 Benefit Harm 0 2 4 6 Time (hours) Saver, Stroke 2006
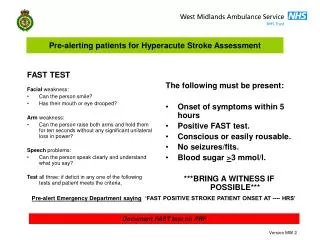
Inclusion criteria • Clinical symptoms and signs of definite acute stroke • Clear time of onset • Presentation within 3 hrs of acute onset • Haemorrhage excluded by CT scan • Age 18 - 80 years old • NIHSS less than 25 • Consent to treat (every effort must be made to contact next of kin)
Rapidly improving or minor stroke symptoms Stroke or serious head injury 3 months Major surgery, obstetrical delivery, external heart massage last 14 days, Seizure at onset of stroke Prior stroke and concomitant diabetes Severe haemorrhage last 21/7 Increase bleeding risk History of central nervous damage (neoplasm, haemorrhage, aneurysm, spinal or intracranial surgery or haemorrhagic retinopathy) Symptoms suggestive of SAH (even if CT is normal) *Blood pressure above 185 mmHg systolic or 110 mmHg diastolic Known clotting disorder Patient on heparin or warfarin Suspected iron deficient anaemia or thrombocytopenia Suspected hypoglycaemia or hyper glycaemia >3 mmol/l > 22 mmol/l Bacterial endocarditis, pericarditis Acute pancreatitis Premorbid dependency Ulcerative GI disease last 3 months, oesophageal varices, arterial-aneurysm, arterial/venous malformation. Severe liver disease including cirrhosis, acute hepatitis Neoplasm with increased bleeding risk Large hypodensity on CT scan (use ASPECTS* scoring if time permits; otherwise use the 1/3 of MCA territory rule) Symptoms suggestive of SAH (even if CT is normal) *Blood pressure above 185 mmHg systolic or 110 mmHg diastolic Known clotting disorder Patient on heparin or warfarin Suspected iron deficient anaemia or thrombocytopenia Suspected hypoglycaemia or hyper glycaemia >3 mmol/l > 22 mmol/l Bacterial endocarditis, pericarditis Acute pancreatitis Premorbid dependency Ulcerative GI disease last 3 months, oesophageal varices, arterial-aneurysm, arterial/venous malformation. Exclusion criteria
Low density loss of grey/white definition loss of insula loss of basal ganglia Hyperdense artery Swelling loss of sulci effacement of ventricles Farrall, Kane, Wardlaw
Conditions • Acute stroke unit • Under the care of stroke physician or neurologist • Monitored bed • Nurses trained in thrombolysis & acute skills • Protocols & guidelines for care • Access to immediate imaging (24hrs)
Hyperacute stroke specialist teams
Patient has Video Consultation with the consultant following viewing of CT brain image -
Network of acute sites (with CT scanning) and stroke specialists
Use of rt-PA for acute ischaemic stroke ‘within licence’ in Europe (SITS-MOST registry 2007) SITS-MOST 29/1/2007
Section Data itemBaselineTreatment file namePostcodeCHI numberAgeGenderSITS-MOST patientDate/time stroke onsetDate/time arrival 1st hospitalDate/time arrival Rx hospitalDate/time brain imaging examDate/time brain imaging reportDate/time of rt-PA treatmentRankin before strokeHypertensionDiabetesHyperlipidaemiaCurrent smokerPrevious smokerPrevious diagnosis of strokeAtrial fib (incl. Paroxysmal)Congestive heart failureNumber of risk factorsAspirin at stroke onsetDipyridamole at stroke onsetClopidogrel at stroke onsetOther antiplatelet at stroke onsetAnticoagulants, high doseAnticoagulants, low doseAnticoagulants, oralAntihypertensive at stroke onsetAntihypertensive oralGlucose before treatmentTotal serum cholesterol level within 24h of stroke onsetCurrently partic. In stroke RCTMethod of consultation [a]Brain imaging review [b]ADRCause of ADR is reasonable related to Actilyse treatmentType of ADRDate SADR faxed to BIIntensity of ADRDate/time of onset of ADRSpecify reaction [c]Treatment file nameSITS-MOST patientAgeGenderCause of ADR is reasonable related to Actilyse treatmentType of ADRDate SADR faxed to BIIntensity of ADRCriteria of serious ADRDate/time of onset of ADRSpecify reactionSerious AD report form DeathTreatment file nameSITS-MOST patientAgeGenderDate of deathPrimary cause of deathCause of death reasonable related to Actilyse treatmentAdd. info. related to deathSerious AD report formNIH stroke scale - BeforeNIH done – before treatmentIf NIH done – total scoreSystolic BPDiastolic BPNIH items 1-11NIH total (calculated)NIH stroke scale – At 2hNIH done – at 2hSystolic BPDiastolic BPNIH items 1-11NIH total (calculated)NIH stroke scale – At 24hNIH done – at 24hSystolic BPDiastolic BPNIH items 1-11NIH total (calculated)NIH stroke scale – At 7dNIH done – at 7dSystolic BPDiastolic BPNIH items 1-11NIH total (calculated)ImagingCT doneCT date/timeCT current infarctCT dense artery signCTA occlusion (optional)CT perfusion deficit (optional)CT perfusion deficit volume optCT infarct volume (optional)CT perfusion/infarct mismatch (optional)CT local haemorrhageCT remote haemorrhageCT volume PH2CT cerebral oedemaMR doneMR date/timeMR current infarctMR artery occlusionMR perfusion deficit (optional)MR diffusion volume (optional)MR perfusion/infarct mismatch (optional)MR local haemorrhageMR remote haemorrhageMR volume PH2MR cerebral oedemaBrain Imaging result [d]TCD occlusionTCD date/timeTreatmentTreatment file nameSITS-MOST patientAgeGenderHas patient received treatment with ActilyseDose mgEstimated weight (kilos)Measured weight (kilos)Reason why no treatment was given [e]Full dose given (0.9mg/kg)Reason why full dose was not given24hTreatment file nameSITS-MOST patientAgeGenderGlobal outcome 24h after start of rt-PA treatment [f]DischargeTreatment file nameSITS-MOST patientAgeGenderAspirin since admissionDipyridamol since admissionClopidogrel since admissionOther antiplatelet since admissionAnticoagulants, high doseAnticoagulants, low doseAnticoagulants, oralAntihypertensive, ivAntihypertensive, oralI-national class of diseases(ICD)Repeat brain imaging done [g]Repeat brain imaging result [h]Global outcome on discharge /7dGlobal outcome on discharge /7d [i] ?Total serum cholesterol level at 7 days of stroke onset, mg/dl3 month follow upTreatment file nameSITS-MOST patientAgeGenderRankin 3m months (+/- 10 days) SITS Register
Prospective part Basic common dataset in SSCA Numbers treated Contraindications Time to treatment Complications Outcomes Equity/service issues Retrospective part Jan 2008 – present Multiple local audits Compile basic common dataset Same data as SSCA Same outcomes and analysis Centralised resource SHARE project
Prospective part Basic common dataset in SSCA Numbers treated Contraindications Time to treatment Complications Outcomes Equity/service issues Retrospective part Jan 2008 – present Multiple local audits Compile basic common dataset Same data as SSCA Same outcomes and analysis Centralised resource SHARE project
The promise and challenge of thrombolysis for ischaemic stroke • Promising treatment for a minority of stroke patients • National and international guidelines NICE technology appraisal • Features in Scottish and English stroke strategies • Challenge to deliver in practical and equitable manner • Need to monitor developments in Scotland