otitis externa oe
Anatomy and Physiology. Consists of the auricle and EAMSkin-lined apparatusApproximately 2.5 cm in lengthEnds at tympanic membrane. Anatomy and Physiology. Auricle is mostly skin-lined cartilageExternal auditory meatusCartilage: ~40%, Bony: ~60%S-shaped, Narrowest portion at bony-cartilage junction.

otitis externa oe
E N D
Presentation Transcript
1. Otitis Externa (OE) Rima Qudah
Ahmed Al-Momtan
2. Anatomy and Physiology Consists of the auricle and EAM
Skin-lined apparatus
Approximately 2.5 cm in length
Ends at tympanic membrane
3. Anatomy and Physiology Auricle is mostly skin-lined cartilage
External auditory meatus
Cartilage: ~40%, Bony: ~60%
S-shaped, Narrowest portion at bony-cartilage junction
4. Anatomy and Physiology EAC is related to various contiguous structures
Tympanic membrane
Mastoid
Glenoid fossa
Cranial fossa
Infratemporal fossa
5. Anatomy and Physiology Innervation: cranial nerves V, VII, IX, X, and greater auricular nerve
Arterial supply: superficial temporal, posterior and deep auricular branches
Venous drainage: superficial temporal and posterior auricular veins
Lymphatics
6. Anatomy and Physiology Squamous epithelium
Bony skin � 0.2mm
Cartilage skin
0.5 to 1.0 mm
Apopilosebaceous unit
7. Otitis Externa Bacterial, viral or fungal infection of external auditory canal
Categorized by time course
Acute
Chronic
8. Speculum findings: the canal may be so swollen that a view into the ear is impossible
In swimmers, divers and surfers, chronic water exposure can lead to the growth of bony swellings in the canal known as exostoses. These can interfere with the drainage of wax and predispose to infection.
9. Differential diagnoses: Otitis media
Ramsay Hunt syndrome
Furuncle
Skull base osteomyelitis
Preauricular cyst and fistula
Lacerations
Atopic dermatitis
Cerumen impaction
Exostosis and osteoma
Foreign body
Acute (bullous) and chronic (granular) myringitis Ramsay Hunt syndrome:
This condition, more accurately known as herpes zoster oticus, is caused by varicella-zoster viral infection. Ramsay Hunt syndrome is characterized by facial nerve paralysis and sensorineural hearing loss, with bullous myringitis and a vesicular eruption of the concha of the pinna and the EAC. A painful otitis externa may be present as well. Treatment includes use of an antiviral agent (eg, valacyclovir) and systemic steroids. The role of facial nerve decompression remains controversial.
Furuncle:
Staphylococcal infection of a hair follicle is the usual cause of a furuncle. This infection occurs in the lateral cartilaginous hair-bearing portion of the EAC. On otoscopic examination, a furuncle is a localized infection, which may develop into an abscess, rather than the diffuse inflammatory process characteristic of otitis externa.
Skull base osteomyelitis:
This serious infection, also known as malignant otitis externa, occurs most often in patients who are diabetic or immunocompromised. The pathogenic bacteria are usually Pseudomonas aeruginosa. Other predisposing conditions include arteriosclerosis, immunosuppression, chemotherapy, steroid use, and other immunodeficient states. The diagnosis is strongly suggested by a history of diabetes mellitus, severe otalgia, cranial neuropathies, and characteristic EAC findings.The EAC may be filled with friable granulation tissue, which is primarily found inferiorly. Because this presentation may be identical to that of a soft tissue malignancy, prudence dictates a tissue biopsy, even if a history of diabetes mellitus is present. Bare bone of the EAC floor may be exposed; small bony sequestra may be observed as well.CT scanning demonstrates bone erosion, and gallium scanning can be performed at points throughout treatment to monitor resolution. Treatment consists of administration of an antipseudomonal IV antibiotic such as ceftazidime (in some cases) or oral ciprofloxacin (in less dramatic cases). Extended treatment for at least 6 weeks is most appropriate. Hyperbaric oxygen therapy may also be effective. Surgical debridement is reserved for granulation tissue and bony sequestra.
Preauricular cyst and fistula:
Abnormal development of the first and second branchial arch may result in the formation of a preauricular cyst or fistula, which may manifest as persistent discharge or recurrent infection. A draining sinus may be present anterior to the tragus; when infected, the cyst distends with pus and the overlying skin is erythematous. These lesions are managed by complete surgical excision if they become repeatedly infected. The facial nerve is at risk of injury during the excision of these lesions because of the close relationship of the preauricular cyst or fistula to the superior branches of the facial nerve within the parotid gland.First branchial cleft anomalies have a more complex embryologic origin than preauricular cysts and fistulas. These lesions may not have an obvious sinus tract on the skin and may manifest as an abscess extending deeply into the EAC, parotid, and/or neck.
Lacerations:
Full-thickness auricular lacerations may be observed after blunt or sharp trauma. These injuries are managed surgically by closing both the perichondrium and the skin. In contrast, external canal lacerations may occur after attempts at cleaning the ear canal using cotton-tipped applicators. These lacerations are usually managed by microscopically placing any skin flaps in their normal position, packing the ear canal, and administering topical antibiotic drops.
Atopic dermatitis:
Drug sensitivity to topical antibiotic solutions is well known. Neomycin allergy occurs in up to 5% of patients treated with the medication. Suspect drug sensitivity if worsening of symptoms associated with skin excoriation and weeping occurs in the distribution of the topical medication exposure after application of drops.Metal sensitivity also manifests as excoriation, erythema, and edema around the exposure site (eg, a piercing hole). A common allergen is nickel, an impurity that may be present in precious metals. Atopic dermatitis is managed by removal of the allergen, such as an earring, and beginning topical steroid and antibiotics if the wound is secondarily infected. The diagnosis of metal sensitivity is confirmed by performing a skin patch test.
Cerumen impaction:
Cerumen impaction is the most common abnormality found on otoscopic examination, yet only a small proportion of the general population requires regular disimpaction because the EAC has the innate ability to produce and clear itself of cerumen. Cerumen may vary in color and consistency and may exist with other pathologies. Of note, debris in the EAC from cholesteatoma or tumors may be confused with cerumen, indicating that considerable care is required when attempting debridement of the EAC. Debridement may be accomplished with microinstruments or by aspirating the ear canal contents with a No 5 or No 7 Barton suction, while under direct vision through the otoscope or microscope. Irrigation of the ear canal is another option, but use of a pressurized irrigation system entails the risk of trauma.
Exostosis and osteoma:
The 2 most common bony lesions of the EAC, exostoses and osteomas, differ histologically and clinically. Exostoses tend to arise from the anterior and/or posterior floor of the medial EAC. Exostoses have a sessile base and are covered with normal-appearing skin. Both anterior and posterior exostoses may be found simultaneously.Osteomas may arise from any region of the bony EAC and often are pedunculated. Osteomas may also be either single or multiple and are covered by normal skin. Exostosis and osteomas require surgical treatment only if they are so large that they lead to a conductive hearing loss or intractable otitis externa.
Foreign body:
Foreign bodies are not infrequently encountered in the EAC. In children, parts of toys or even food may be found in the EAC, and, thus, appearance varies. In adults, fragments of cotton swabs are the most common finding. Erythema and edema surrounding the foreign body are commonly present. Using microinstruments, the foreign body may be removed under a microscope, depending on the patient's ability to cooperate.
Acute (bullous) and chronic (granular) myringitis:
Acute myringitis is usually caused by a mycoplasma or viral infection and is observed in adults and children. It is characterized by hemorrhagic bullae involving the tympanic membrane and a flulike syndrome. It is self-limiting and requires pain and fever management.Chronic myringitis is defined as deepithelization of the tympanic membrane, granulation tissue formation, and discharge. Treatment includes topical application of eardrops, a caustic solution in unresponsive cases, and mechanical removal of polypoidal granulations.Ramsay Hunt syndrome:
This condition, more accurately known as herpes zoster oticus, is caused by varicella-zoster viral infection. Ramsay Hunt syndrome is characterized by facial nerve paralysis and sensorineural hearing loss, with bullous myringitis and a vesicular eruption of the concha of the pinna and the EAC. A painful otitis externa may be present as well. Treatment includes use of an antiviral agent (eg, valacyclovir) and systemic steroids. The role of facial nerve decompression remains controversial.
Furuncle:
Staphylococcal infection of a hair follicle is the usual cause of a furuncle. This infection occurs in the lateral cartilaginous hair-bearing portion of the EAC. On otoscopic examination, a furuncle is a localized infection, which may develop into an abscess, rather than the diffuse inflammatory process characteristic of otitis externa.
Skull base osteomyelitis:
This serious infection, also known as malignant otitis externa, occurs most often in patients who are diabetic or immunocompromised. The pathogenic bacteria are usually Pseudomonas aeruginosa. Other predisposing conditions include arteriosclerosis, immunosuppression, chemotherapy, steroid use, and other immunodeficient states. The diagnosis is strongly suggested by a history of diabetes mellitus, severe otalgia, cranial neuropathies, and characteristic EAC findings.The EAC may be filled with friable granulation tissue, which is primarily found inferiorly. Because this presentation may be identical to that of a soft tissue malignancy, prudence dictates a tissue biopsy, even if a history of diabetes mellitus is present. Bare bone of the EAC floor may be exposed; small bony sequestra may be observed as well.CT scanning demonstrates bone erosion, and gallium scanning can be performed at points throughout treatment to monitor resolution. Treatment consists of administration of an antipseudomonal IV antibiotic such as ceftazidime (in some cases) or oral ciprofloxacin (in less dramatic cases). Extended treatment for at least 6 weeks is most appropriate. Hyperbaric oxygen therapy may also be effective. Surgical debridement is reserved for granulation tissue and bony sequestra.
Preauricular cyst and fistula:
Abnormal development of the first and second branchial arch may result in the formation of a preauricular cyst or fistula, which may manifest as persistent discharge or recurrent infection. A draining sinus may be present anterior to the tragus; when infected, the cyst distends with pus and the overlying skin is erythematous. These lesions are managed by complete surgical excision if they become repeatedly infected. The facial nerve is at risk of injury during the excision of these lesions because of the close relationship of the preauricular cyst or fistula to the superior branches of the facial nerve within the parotid gland.First branchial cleft anomalies have a more complex embryologic origin than preauricular cysts and fistulas. These lesions may not have an obvious sinus tract on the skin and may manifest as an abscess extending deeply into the EAC, parotid, and/or neck.
Lacerations:
Full-thickness auricular lacerations may be observed after blunt or sharp trauma. These injuries are managed surgically by closing both the perichondrium and the skin. In contrast, external canal lacerations may occur after attempts at cleaning the ear canal using cotton-tipped applicators. These lacerations are usually managed by microscopically placing any skin flaps in their normal position, packing the ear canal, and administering topical antibiotic drops.
Atopic dermatitis:
Drug sensitivity to topical antibiotic solutions is well known. Neomycin allergy occurs in up to 5% of patients treated with the medication. Suspect drug sensitivity if worsening of symptoms associated with skin excoriation and weeping occurs in the distribution of the topical medication exposure after application of drops.Metal sensitivity also manifests as excoriation, erythema, and edema around the exposure site (eg, a piercing hole). A common allergen is nickel, an impurity that may be present in precious metals. Atopic dermatitis is managed by removal of the allergen, such as an earring, and beginning topical steroid and antibiotics if the wound is secondarily infected. The diagnosis of metal sensitivity is confirmed by performing a skin patch test.
Cerumen impaction:
Cerumen impaction is the most common abnormality found on otoscopic examination, yet only a small proportion of the general population requires regular disimpaction because the EAC has the innate ability to produce and clear itself of cerumen. Cerumen may vary in color and consistency and may exist with other pathologies. Of note, debris in the EAC from cholesteatoma or tumors may be confused with cerumen, indicating that considerable care is required when attempting debridement of the EAC. Debridement may be accomplished with microinstruments or by aspirating the ear canal contents with a No 5 or No 7 Barton suction, while under direct vision through the otoscope or microscope. Irrigation of the ear canal is another option, but use of a pressurized irrigation system entails the risk of trauma.
Exostosis and osteoma:
The 2 most common bony lesions of the EAC, exostoses and osteomas, differ histologically and clinically. Exostoses tend to arise from the anterior and/or posterior floor of the medial EAC. Exostoses have a sessile base and are covered with normal-appearing skin. Both anterior and posterior exostoses may be found simultaneously.Osteomas may arise from any region of the bony EAC and often are pedunculated. Osteomas may also be either single or multiple and are covered by normal skin. Exostosis and osteomas require surgical treatment only if they are so large that they lead to a conductive hearing loss or intractable otitis externa.
Foreign body:
Foreign bodies are not infrequently encountered in the EAC. In children, parts of toys or even food may be found in the EAC, and, thus, appearance varies. In adults, fragments of cotton swabs are the most common finding. Erythema and edema surrounding the foreign body are commonly present. Using microinstruments, the foreign body may be removed under a microscope, depending on the patient's ability to cooperate.
Acute (bullous) and chronic (granular) myringitis:
Acute myringitis is usually caused by a mycoplasma or viral infection and is observed in adults and children. It is characterized by hemorrhagic bullae involving the tympanic membrane and a flulike syndrome. It is self-limiting and requires pain and fever management.Chronic myringitis is defined as deepithelization of the tympanic membrane, granulation tissue formation, and discharge. Treatment includes topical application of eardrops, a caustic solution in unresponsive cases, and mechanical removal of polypoidal granulations.
10. Organisms Pseudomonas species
Staphylococci
Streptococci/Gram negative rods
Fungi (Aspergillus/Candida species)
11. Labs/workup Usually after failed empiric therapy:
bacterial and fungal culture
Adults with otitis externa: screening blood glucose and/or a urine dipstick test to rule out occult diabetes.
Additional tests (if available):
Gram stain of d/c
KOH prep smear (within 10 min)
13. Acute Otitis Externa (AOE) �swimmer�s ear�
Preinflammatory stage
Acute inflammatory stage
Mild
Moderate
Severe
14. Factors contributing to AOE High humidity
Water exposure
Maceration of canal skin
High environmental temperature
Local trauma
Perespiration
Allergy
Stress
Removal of normal skin lipids
Absence of cerumen
Alkaline pH of canal In the early stages of EO, heat, humidity, maceration, or other factors may act to remove cerumen or change the pH of the canal. These changes may cause itching that then elicits digital manipulation or instrumentation of the canal that traumatizes the skin, thus allowing bacteria to enter the surrounding soft tissue.
An increase in infection and iflammation may cause canal oedema or complete obstruction of the canal in sever cases.In the early stages of EO, heat, humidity, maceration, or other factors may act to remove cerumen or change the pH of the canal. These changes may cause itching that then elicits digital manipulation or instrumentation of the canal that traumatizes the skin, thus allowing bacteria to enter the surrounding soft tissue.
An increase in infection and iflammation may cause canal oedema or complete obstruction of the canal in sever cases.
15. AOE: Preinflammatory Stage Oedema of stratum corneum and plugging of apopilosebaceous unit
Symptoms: pruritus and sense of fullness
Signs: mild edema
Starts the itch/scratch cycle
16. AOE: Mild to Moderate Stage Progressive infection
Symptoms
Pain
Increased pruritus
Signs
Erythema
Increasing edema
Canal debris, discharge
17. AOE: Severe Stage Severe pain, worse with ear movement
Signs
Lumen obliteration
Purulent otorrhoea
Involvement of periauricular soft tissue
18. AOE: Treatment Most common pathogens: P. aeruginosa and S. aureus, E.coli and proteus.!
Four principles
Frequent canal cleaning; swap or suction
With sever EO, palcement of a wick made of sponge or gauze provides a pathway for drops to be delivered to the EAC wall skin for 48-72 hours!
Topical antibiotics, and if sever>> Systemic PO,ABT
Pain control
Instructions for prevention
19. AT A GLANCE. . . Ostalgia
Tenderness on palpation or manipulation (tragus sign)
Ear fullness
Conductive hearing loss.
Erythaema of meatus and canal
Swelling and obstruction of canal
Crusting and discharge
Odor!
20. Furunculosis Acute localized infection
Lateral 1/3 of posterosuperior canal
Obstructed apopilosebaceous unit
Pathogen: S. aureus -lateral one third >> hair bearing portion of the canal.
-lateral one third >> hair bearing portion of the canal.
21. Furunculosis: Symptoms Localized pain
Pruritus
Hearing loss (if lesion occludes canal)
22. Furunculosis: Signs Edema
Erythema
Tenderness
Occasional fluctuance
Localized furucle infection but may proress into an abscess.Localized furucle infection but may proress into an abscess.
23. Furunculosis: Treatment Local heat
Analgesics
Oral anti-staphylococcal antibiotics
Incision and drainage reserved for localized abscess
IV antibiotics for soft tissue extension
- tri-adcortyle! Nystatine, neomycine,gramicidine, triamsonolone
- Iv-24h / flucloxacillinNystatine, neomycine,gramicidine, triamsonolone
- Iv-24h / flucloxacillin
24. Erysipelas Acute superficial cellulitis
Group A, beta hemolytic streptococci
Skin: bright red; well-demarcated, advancing margin
Rapid treatment with oral or IV antibiotics if insufficient response
25. Otomycosis Mostly in children who are exposed to warm, moist climates or who have a Hx of chronic use of antibiotic ear drops.
Fungal infection of EAC skin
Primary or secondary
Most common organisms: Aspergillus and Candida Both the moisture and ab alter the cerumen and normal bacterial flora of the EAC.
These black dots (spores) are the appearance of fungal infection (aspergillus niger), with other fungi the spores may be white or yellow
chronic otitis externa: Although the canal wall is not swollen, the skin is excoriated and red. The drum is essentially normal.
Both the moisture and ab alter the cerumen and normal bacterial flora of the EAC.
These black dots (spores) are the appearance of fungal infection (aspergillus niger), with other fungi the spores may be white or yellow
chronic otitis externa: Although the canal wall is not swollen, the skin is excoriated and red. The drum is essentially normal.
26. Otomycosis: Symptoms
27. Otomycosis: Treatment Thorough cleaning and drying of canal
Topical antifungals (clotrimazole for eg., amphotericine B, oxytetracycline-polymyxin, and nystatin are very effective!)
Acidifying of the EAC with drops like 2% acetic acid, 3% boric acid or sulzberger�s powder are also helpful in the t/t of fungal infections.
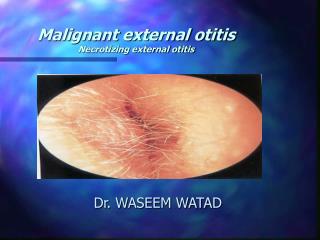
28. Necrotizing (malignant) External Otitis(NEO) Potentially lethal infection of EAC and surrounding structures
Pseudomonas aeruginosa is the usual culprit
Risk Factors:
- Diabetes Mellitus
- Elderly
- Immunocompromised state
- Human Immunodeficiency Virus (HIV)
Typically seen in diabetics and immunocompromised patients
29. NEO: Signs & Symptoms Similar to Otitis Externa except
Severe, unrelenting Ear Pain and Headache
Persistent discharge
Does not respond to topical medications
Commonly associated with Diabetes Mellitus
Granulation tissue in posterior and inferior canal
Pathognomonic for necrotizing otitis
Occurs at bone-cartilage junction
Extra-auricular findings
Cervical Lymphadenopathy
Trismus (TMJ involvement)
Facial Nerve Palsy or paralysis (Bell's Palsy)
Associated with poor prognosis
30. NEO: Dx, Prevention and T/T: Prognosis; Reportedly mortality 20-53%
Dx: Hx, PE, Labs and Imaging:
Labs; FBC, Culture of discharge, ESR, Serum glucose, Serum creatinine.
Radiology; CT, or MRI (ear),Tc 99m medronate methylene bone scanning, Ga 67 scintography.
Prevention:
Avoid use of cotton swabs in ear and other canal trauma.
Use caution when irrigating ear of high risk patients.
Treat eczema of ear canal and other pruritic dermatitis Some may aquire histo o granulation tissue.
Galium has high sensitivity for current infx, and usefull for F/U.Some may aquire histo o granulation tissue.
Galium has high sensitivity for current infx, and usefull for F/U.
31. NEO: Treatment Intravenous antibiotics for at least 4 weeks � with serial gallium scans monthly
Local canal debridement until healed
Pain control
Use of topical agents controversial
Hyperbaric oxygen experimental
Surgical debridement for refractory cases Admit to hospital
Anti-pseudomonal antibiotics
Intravenous Antibiotic options
Ciprofloxacin 400 mg IV q12 hours
Imipenem 0.5 mg IV q6 hours
Meropenem 1.0 grams IV q8 hours
Ceftazidime 2.0 grams IV q8 hours
Cefepime 2.0 grams IV q12 hours
Gentamicin 1 to 1.66 mg/kg IV or IM/IV with
Ticarcillin or
Piperacillin
Timentin 3.0 grams IV q4 hours
Oral antibiotic options (after initial IV course)
Ciprofloxacin 750 mg PO q12 hours
Course
Start with IV antibiotics
Continue antibiotics for 4-8 weeks
Consult Otolaryngology (ENT)
Surgical debridement may be required
Clean ear canals meticulously on a daily basis
Clean and debride canal
Apply topical antibiotic agents
Other modalities to consider
Hyperbaric oxygen chamberAdmit to hospital
Anti-pseudomonal antibiotics
Intravenous Antibiotic options
Ciprofloxacin 400 mg IV q12 hours
Imipenem 0.5 mg IV q6 hours
Meropenem 1.0 grams IV q8 hours
Ceftazidime 2.0 grams IV q8 hours
Cefepime 2.0 grams IV q12 hours
Gentamicin 1 to 1.66 mg/kg IV or IM/IV with
Ticarcillin or
Piperacillin
Timentin 3.0 grams IV q4 hours
Oral antibiotic options (after initial IV course)
Ciprofloxacin 750 mg PO q12 hours
Course
Start with IV antibiotics
Continue antibiotics for 4-8 weeks
Consult Otolaryngology (ENT)
Surgical debridement may be required
Clean ear canals meticulously on a daily basis
Clean and debride canal
Apply topical antibiotic agents
Other modalities to consider
Hyperbaric oxygen chamber
32. NEO: Diagnosis Cohen and Friedman � criteria from review: They were divided into two categories: obligatory and occasional. The obligatory criteria are: pain, edema, exudate, granulations, microabscess (when operated), positive bone scan or failure of local treatment often more than 1 week, and possibly pseudomonas in culture. The occasional criteria are diabetes, cranial nerve involvement, positive radiograph, debilitating condition and old age. All of the obligatory criteria must be present in order to establish the diagnosis. The presence of occasional criteria alone does not establish it. The importance of Tc99 scan in detecting osteomyelitis is stressed. When bone scan is not available, a trial of 1-3 weeks of local treatment is suggested. Failure to respond to such treatment may assist in making the diagnosis of MEO.
33. NEO: Mortality Death rate essentially unchanged despite newer antibiotics (37% to 23%)
Higher with multiple cranial neuropathies (60%)
Recurrence not uncommon (9% to 27%)
May recur up to 12 months after treatment
34. Perichondritis/Chondritis Infection of perichondrium/cartilage
Result of trauma to auricle
May be spontaneous (overt diabetes)
Usual pathogens include pseudomonas species and mixed flora
Blood and/or serum collects in the potential space between the cartilage and perichondrium and infection of this fluid results in perichondritis and chondritis.
Blood and/or serum collects in the potential space between the cartilage and perichondrium and infection of this fluid results in perichondritis and chondritis.
35. Perichondritis: Symptoms Pain over auricle and deep in canal
fever
Pruritus
36. Perichondritis: Treatment Aspiration of the pus
Use antibiotics of gram-negative coverage, specifically anitpseudomonals.
If frank chondritis develops, incisions should be made in the cartilage in order to provide adequate drainage.
Mild: debridement, topical & oral antibiotic
Advanced: hospitalization, IV antibiotics
Chronic: surgical intervention with excision of necrotic tissue and skin coverage
37. Relapsing Polychondritis Uncommon progressive inflammatory disorder that may affect children, but more commonly in adults.
Episodic and progressive inflammation of cartilages
Autoimmune etiology?
External ear, larynx, trachea, bronchi, and nose may be involved
Involvement of larynx and trachea causes increasing respiratory obstruction Destruction of the cartilage due to inflammatory infiltrates is often followed by granulation and then fibrosis and calcificationDestruction of the cartilage due to inflammatory infiltrates is often followed by granulation and then fibrosis and calcification
38. Relapsing Polychondritis Fever, pain
Swelling, erythaema
Arthralgia!
Tenderness of the nasal septum may progress to complete destruction of the septum Destruction of the septum ultimately lead to a nasal-suddle deformity in some cases.
DDx: rheumatoid arthritis (juvnile)
lymphoma
or infectious perichondritis
Destruction of the septum ultimately lead to a nasal-suddle deformity in some cases.
DDx: rheumatoid arthritis (juvnile)
lymphoma
or infectious perichondritis
39. Dx and T/t Weak +ve RF
ANA +ve
High ESR,
Anaemia
And difinitve Dx is made by a biopsy from the affected cartilage
40. Herpes Zoster Oticus(Ramsay Hunt Syndrome) J. Ramsay Hunt described in 1907
Viral infection caused by varicella zoster
Infection along one or more cranial nerve dermatomes (shingles).
herpes zoster of the pinna with otalgia.
facial paralysis
sensorineural hearing loss
Bullus myringitis
A vesicular eruption of the concha of the pinna and the EAC.
41. Symptoms Early: burning pain in one ear, headache, malaise and fever
Late (3 to 7 days): vesicles, facial paralysis
42. Bullous Myringitis Viral infection
Confined to tympanic membrane
Primarily involves younger children
43. Bullous Myringitis: Symptoms Sudden onset of severe pain
No fever
No hearing impairment
Bloody otorrhoea (significant) if rupture
44. Bullous Myringitis: Treatment Self-limiting
Analgesics
Topical antibiotics to prevent secondary infection
Incision of blebs is unnecessary
45. Chronic Otitis Externa Acute otitis externa occurs in 4 of every 1000 people per year
Otitis externa is defined as chronic when the duration of the infection exceeds 4 weeks or when more than 4 episodes occur in 1 year
Bacterial, fungal, dermatological aetiologies
46. COE: Signs Asteatosis
Dry, flaky skin
Hypertrophied skin
Mucopurulent otorrhoea (occasional)
47. COE: Treatment Similar to that of AOE
Topical antibiotics, frequent cleanings
Topical Steroids
Surgical intervention
Failure of medical treatment
Goal is to enlarge and resurface the EAC
48. Radiation-Induced Otitis Externa OE occurring after radiotherapy
Often difficult to treat
Limited infection treated like COE
Involvement of bone requires surgical debridement and skin coverage
49. Granular Myringitis (GM) Deepithelization of the TM
Localized chronic inflammation of pars tensa with granulation tissue
Sequela of primary acute myringitis, previous OE, perforation of TM
Common organisms: Pseudomonas, Proteus
50. GM: Symptoms Foul smelling discharge from one ear
Often asymptomatic
Slight irritation or fullness
No hearing loss or significant pain
51. GM: Treatment Careful and frequent debridement
Topical anti-pseudomonal antibiotics
Occasionally combined with steroids
At least 2 weeks of therapy
May warrant careful destruction of granulation tissue if no response
52. Eczema External clue to OE (atopic, contact and sebrrheoic) dermatitis
Usual symptom is itching.
P/E; erythaema, oedema, flaking and crusting.
T/t:
Local cleansing.
Usage of corticosteroid and drying agents.
Metal sensitivity is the most common form of chronic dermatitis involving the ear.!
Nickel is the most common offending metal.
Women are affected more than men.
- Ear peircing is an important cause of primary sensitization to nickel.
53. Conclusions Careful History
Thorough physical exam
Understanding of various disease processes common to this area
Vigilant treatment and patience
54. Questions/Comments?