Download
1 / 13
130 likes | 150 Vues
Explore symptoms associated with lesions in sensory pathways, from dorsal column system to trigeminal and cerebellar tracts. Learn about Tabes Dorsalis, Syringomyelia, Wallenberg's Syndrome, and more.

E N D
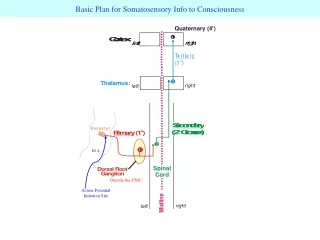
Basic Plan for Somatosensory Info to Consciousness o Quaternary (4 ) Action Potential Initiation Site 4 3 2 1 Outside the CNS!
Dorsal Column System – Symptoms Associated with Lesions What is the symptom associated with the lesion?
Lateral Spinothalamic Tract – Symptoms Associated with Lesions
Cerebellar Tracts: Non-Conscious Proprioception DorsalSpinocerebellarTract CuneocerebellarTract Anterior Lobe Posterior Lobe Paramedian Lobule Flocculonodular Lobe Cerebellar Nuclei Dorsal Spino- CerebellarTract Cuneo- CerebellarTract Inferior Cerebellar Peduncle Restiform Body o Secondary 2 e s p T1 to L2 a Spinal Cord: n y Dorsal Nucleus of Clarke s C2 to T4 o DRG DRG DRG Primary 1 Receptor Receptor Receptor Medulla
Lesions and Clinical Deficits – Tabes Dorsalis Area of Lesion Degeneration of myelinated afferent fibers in the dorsal columns, (destroys large diameter axons), is a late stage of syphilis. Symptoms: Severe deficits in touch and position sense but often little loss of temperature perception and of nociception. Bilateral lesion = bilateral effects.
Lesions and Clinical Deficits - Syringomyelia Gliosis and cavitation in midline of the spinal cord – CSF enters the cord. The larger the cavitation, the more tracts affected. One possible cause is a Chiari Malformation. Other causes include trauma, infection. (anything that compresses the CSF) Symptoms: Bilateral loss of pain and temperature at the level of the lesion (segments involved). Area of lesion http://www.asap4sm.com/
Lesions and Clinical Deficits - Wallenberg’s Spinal Trigeminal Tract Trigeminal Nucleus Dorsal Spinocerebellar Tract Ventral Spinocerebellar Tract ALS (lateral spinothalamic tract) Lateral Medullary (Wallenberg’s) Syndrome – Symptoms include loss of pain and temperature on the ipsilateral head/face, contralateral loss of pain and temperature in the body, and ataxia.
LESIONS and Clinical Deficits – Brown-Sequard Syndrome Hemisection of the spinal cord, often in the cervical spinal cord – (it is rare for the entire hemisection to be affected, but this does occur, more often incomplete hemisection is found). Symptoms: a) Loss of fine discrimination touch, vibration, and position sense ipsilaterally for body regions from affected dermatome and down b) Loss of pain and temperature contralaterally for body regions from affected dermatome and down (small region of bilateral loss of pain and temp at level of lesion and 2 segments below) c) Motor Effects: – Ipsilateral Spasticity and Weakness DC Arch Neurol (2001) 58: 1470.
Approach to starting from symptoms Body Head Trigeminal System/Pathway What modalities? Pain & temp only Fine Discrimination Touch only Spinal Trigeminal tract (ipsi) or Spinal Trigeminal nucleus (ipsi) or VTT (Ventral Trigeminothalamic Tract (contra) Main Trigeminal Nucleus (ipsi) all modalities focal = Trigeminal ganglion (ipsi) all modalities entire face – VPM (ventral posterior medial nucleus of the thalamus) (contra)
Approach to starting from symptoms Body Head Which modality? pain & temp only nonconscious proprioception ataxia, cluminess Fine discrimination touch only ALS dorsal column - medial lemniscus pathway spinocerebellar tracts/pathways widespread or focal? widespread (entire body) – but without other modalities lateral spinothalamic tract (contra) widespread (entire body) medial lemniscus (contra) focal – spinal cord – dorsal funiculus (ipsi) focal or relatively focal – without other modalities – spinal cord – dorsal horn (2o cell bodies) (ipsi) Combination of modalities: If all symptoms are on the same side of the body then it has to be AFTER both pathways have crossed the midline (THUS CONTRA) – so above the medulla. Could be in tracts as they sit next to each other just before they reach the thalamus, or in VPL or in cortex. If it is a loss of touch on one side of the body and a loss of pain & temperature mostly on the other side but with a small region of bilateral pain & temp loss – this is key for spinal cord lesion.