Download

1 / 21
230 likes | 548 Vues
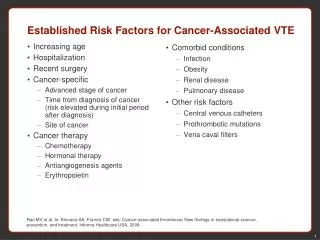
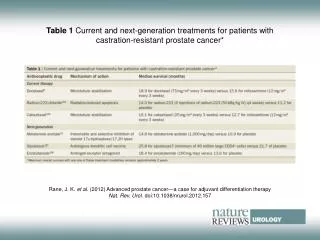
Adjuvant therapy for stage II colon cancer: where are we now?. Professor Werner Scheithauer University of Vienna Vienna, Austria. Healthcare providers. Treatment costs. Resource use. Factors that may influence adjuvant treatment decisions. Patient characteristics. Biomarkers.

E N D
Adjuvant therapy for stage II colon cancer: where are we now? Professor Werner ScheithauerUniversity of ViennaVienna, Austria
Healthcareproviders Treatment costs Resourceuse Factors that may influenceadjuvant treatment decisions Patientcharacteristics Biomarkers Comorbidities e.g. diabetes, impairedcardiac function Disease stage Age Benefit-to-risk ratio Treatmentoutcomes Efficacy Toxicity Impact on lifestyle Patients Convenience Preference
Stage II colon cancer:a heterogeneous population • 28% of diagnosed colon cancer patients • 25–30% of stage II patients will recur within 5 years • Wide spectrum of disease1 • IIa: T3, N0, M0 • IIb: T4, N0, M0 • 5-year DFS2 • IIa: 65–73% • IIb: 51–60% 1. AJCC Cancer Staging Handbook, 6th ed2. Gill S et al. J Clin Oncol 2004;22:1797–806
Adjuvant therapy for stage II colon cancer: the controversy • Lack of definitive data on relative and absolute benefits • Underpowered studies • small numbers of patients • low risk of recurrence • competing non-cancer-related deaths • 4700 patients required for 4% survival benefit1 • Inaccurate staging of patients • number of nodes analysed associated with survival2 • examination of 12 lymph nodes recommended3 1. Benson AB et al. J Clin Oncol 2004;22;3408–192. Le Voyer TE et al. J Clin Oncol 2003;21:2912–93. Fielding LP et al. J Gastroenterol Hepatol 1991;6:325–44
Clinical recommendations for adjuvant treatment of stage II colon cancer • ASCO1 • routine use of adjuvant treatment for stage II disease not recommended • could be considered for patients with inadequately sampled nodes, T4 lesions, perforation or poorly differentiated histology • clinical decision should also be based on extensive discussion with the patient • ESMO2 • adjuvant therapy may be considered in selected node-negative patients 1. Benson et al. J Clin Oncol 2004;22:3408–192. Van Cutsem E et al. Ann Oncol 2005;16(Suppl. 1):i16–7
Adjuvant therapy for stage II colon cancer: evidence against • INT-00351 • IMPACT B22 • ASCO meta-analysis3 1. Moertel CG et al. J Clin Oncol 1995;13:2936–432. IMPACT B2 Investigators. J Clin Oncol 1999;17:1356–633. Benson et al. J Clin Oncol 2004;22:3408–19
INT-0035: non-significant increasein RFS with 5-FU adjuvant therapy 7-yearRFS (%) Estimated probability 1.0 0.8 0.6 0.4 0.2 0 5-FU/LEV (n=159) 79Observation (n=159) 71 Absolute gain: 8% p=0.10 0 1 2 3 4 5 6 7 8 9 10 Years Moertel CG et al. J Clin Oncol 1995;13:2936–43
IMPACT B2: no improvement in survival with adjuvant 5-FU/LV in B2 colon cancer *Event-free survival IMPACT B2 Investigators. J Clin Oncol 1999;17:1356–63
Adjuvant therapy for stage IIcolon cancer: evidence in favour • NSABP 01–041 • Dutch analysis2 • CKVO3 • QUASAR-14 • Japanese meta-analysis5 • MOSAIC6 1. Mamounas E et al. J Clin Oncol 1999;17:1349–552. Taal B et al. Br J Cancer 2001;85:1437–433. Gill S et al. J Clin Oncol 2004;22:1797–8064. Gray RG et al. J Clin Oncol 2004;22(Suppl. 14S):245s (Abst 3501)5. Meta-analysis group. J Clin Oncol 2004;22:484–926. de Gramont et al. J Clin Oncol 2005;23(Suppl. 16S):246s (Abst 3501)
NSABP 01–04: similar benefit after adjuvant therapy for Dukes’ B and C patients All patients Dukes’ B Dukes’ C DEATH MOF vs operation PVI vs operation 5-FU/LV vs MOF 5-FU/LVvs 5-FU/LEV RECURRENCE MOF vs operation PVI vs operation 5-FU/LV vs MOF 5-FU/LVvs 5-FU/LEV DFS EVENT MOF vs operation PVI vs operation 5-FU/LV vs MOF 5-FU/LVvs 5-FU/LEV 0.5 1 2 0.25 0.5 1 2 0.5 1 2 Cumulative odds ratio Mamounas E et al. J Clin Oncol 1999;17:1349–55
Dutch analysis suggests improvedOS for stage II and III disease with 5-FU/LEV 5-yearOS (%) Estimated probability 1.0 0.8 0.6 0.4 0.2 0 5-FU/LEV (n=514) 68Control (n=515) 58 Log-rank p=0.007 0 1 2 3 4 5 6 Years Taal B et al. Br J Cancer 2001;85:1437–43
QUASAR-1: adjuvant therapysignificantly reduces recurrence 5-yearRFS (%) Estimated probability 1.0 0.8 0.6 0.4 0.2 0 Chemotherapy (n=1622) 78Observation (n=1617) 74 Absolute gain: 4% p=0.001 0 1 2 3 4 5 6 7 8 9 10 Years Gray RG et al. J Clin Oncol 2004;22 (Suppl. 14S):245s (Abst 3501)
QUASAR-1: adjuvant therapyimproves OS in stage II Estimated probability 1.0 0.8 0.6 0.4 0.2 0 Chemotherapy (n=1492) Observation (n=1488) Absolute gain: 4% p=0.04 0 1 2 3 4 5 6 7 8 9 10 Years Gray RG et al. J Clin Oncol 2004;22 (Suppl. 14S):245s (Abst 3501)
Japanese meta-analysis: adjuvant oral fluoropyrimidines improve DFS in stage II Favourstreatment Favourscontrol Hazard reduction± SE (%) Dukes’ A 34±18 22±8 Dukes’ B Dukes’ C 11±6 Total 15±4 0 1 2 HR Japanese meta-analysis group. J Clin Oncol 2004;22:484–92
Should high-risk stage II patients be offered adjuvant chemotherapy? • Some high-risk patients may specifically benefit from adjuvant chemotherapy • T4 lesions • poor histological grade (grade 3 or 4 lesions) • peritumoural lymphovascular involvement • bowel obstruction • localised perforation • indeterminate or positive margins • inadequately sampled nodes (<12) NCCN Clinical Practice Guidelines in Oncology v.1.2007
MOSAIC: 5.4% increase in DFSin high-risk stage II patients with FOLFOX4 Estimated probability 1.0 0.9 0.8 0.7 0.6 0 FOLFOX4 (n=286) LV5FU2 (n=290) Absolute gain: 5.4% HR=0.76 0 6 12 18 24 30 36 42 48 Years de Gramont A et al. J Clin Oncol 2005;23(Suppl. 16S):246s (Abst 3501)
Adjuvant therapy for stage II colon cancer: the evidence so far *OS; †high-risk patients
Patients who could benefit arestill denied adjuvant therapy • Indication of benefit of adjuvant therapy in stage II • Some high-risk stage II patients may benefit more than stage III • T4 G3 stage II • older patients may benefit too1 • Better prognostic factors could aid patient selection • rigorous nodal sampling may improve cost-effectiveness2 • Biomarker data collection in most ongoing studies • microsatellite instability • LOH at 18q 1. Leonardi S et al. J Clin Oncol 2006;24(Suppl. 18S):621s (Abst 13564)2. Chen SL et al. Proc ASCO GI 2006 (Abst 370)
Upcoming evidence: ECOG E5202 trial RANDO MIS ATION FOLFOX High-risk MSS with 18q LoHMSI-L with LoH Stage IIcolon cancer(resected <60 days) FOLFOX+Avastin Low-risk MSS with retention of 18q alleles MSI-L with retention of 18q alleles MSI-H with or without retention of 18q alleles Observation
Xeloda: optimal treatment forpatients with stage II disease? • Xeloda has a favourable benefit-to-risk ratio vs5-FU/LV in stage III disease1,2 • consistent efficacy benefits • improved safety • convenient • cost-saving 1. Twelves CJ. Clin Colorectal Cancer 2006;6:278–872. Schmoll H-J et al. J Clin Oncol 2007;25:102–9
Redefining adjuvant therapiesfor stage II patients • Adjuvant chemotherapy provides a small but significant survival benefit • Risks to the patient should be minimised when the benefits are small • Define high-risk groups with increased survival benefit, e.g. T4 vascular invasion, using molecular assays • Xeloda can be considered for stage II patients • based on a favourable benefit-to-risk ratio in stage III disease compared with 5-FU/LV