Download

1 / 69
1.93k likes | 7.29k Vues
Cardiac output: it’s REGULATION AND CONTROL OF CARDIAC FUNCTION. Dr Priyanka. University College of Medical Science s & GTB Hospital, Delhi. INDEX. Definition of cardiac output Determinants of stroke volume Preload –Venous return , EDV Contractility –EF Afterload – PVR &SVR

E N D
Cardiac output: it’s REGULATION AND CONTROL OF CARDIAC FUNCTION Dr Priyanka University College of Medical Science s & GTB Hospital, Delhi
INDEX Definition of cardiac output Determinants of stroke volume Preload –Venous return , EDV Contractility –EF Afterload – PVR &SVR Determinants of Heart Rate sympathetic innervation parasympathetic innervation Control of cardiac function Neural control Hormonal control Cardiac Reflexes
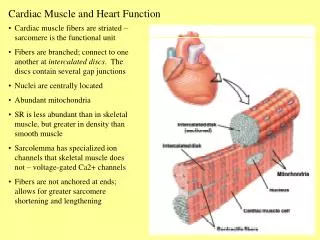
Cardiac output • Amount of blood pumped by each ventricle per minute into circulation • 5-6 l/min • 10-20 % less for females Principle of continuity • Law of conservation of mass--volume of blood ejected by left heart =volume of blood received by right heart
Clinical significance • If RV output increases LV output by 0.1 ml/ minute/beat • Then RV output will increase LV output by 7 ml/minute • In 3 hrs, RV output increases LV output by 7×3×60 =1260 ml This example demonstrates that even small imbalances in stroke volumes of the two hearts could lead to accumulation of blood in one portion of CVS LV output is exactly equal to the RV output
Cardiac index • Measure used to compare cardiac output of different sized individuals • CI = CO/BSA • 2.5 – 3.5 l/min/m2 Stroke volume • Amount of blood pumped by each ventricle per beat • 70 - 90 ml
Control of cardiac output (CO = HR ×SV) • Control of heart rate (extrinsic) • Control of stroke volume(intrinsic)
Control of stroke volume • Heterometric regulation • factors affecting venous return (preload) • Homometric regulation • factors affecting cardiac contractility • Factors affecting afterload
Preload • Ventricular wall stress at end-diastole • Force imposed on a resting muscle i.e. prior to the onset of muscle contraction which stretches the muscle to a new length • Determined by • ventricular EDV • EDP • Wall thickness
Factors affecting preload • Total blood volume • Venous return • Intra thoracic pressure ( thoracic pump) • Cardiac pump • Pumping action of skeletal muscles • Ventricular filling(compliance) • Body position • Intra pericardial pressure
Total blood volume (Clinical implication) Perioperative ventricular hypervolemia ( TBV) Regurgitant valvular heart lesions Ischemic heart disease Viral and idiopathic cardiomyopathy End stage stenotic valvular lesions
Causes of perioperative ventricular hypovolemia ( TBV) Diminished intravascular volume Excessive surgical bleeding Extravasation Excessive diuresis Reduced fluid intake Reduced venous return Increased capacitance (anaesthetics, vasodilators, sympatholytics) increased resistance to venous inflow(PEEP, acute pulmonary HTN, PE, atrial masses, tamponade)
Venous return • Quantity of blood flowing from the veins into the right atrium each minute • CO is controlled by venous return ; heart is not the primary controller of CO • Peripheral factors are more important in controlling cardiac output • Cardiac output regulation is the sum total of all local blood flow regulations • In built mechanism of heart
HETEROMETRIC REGULATION Factors affecting preload and systolic performance • Frank starling law (Described by Otto Frank and Ernest Starling ) length force of cardiac contraction • Effect depends on venous return & is independent of cardiac innervation • In myocardium, actin and myosin filaments are brought to a more optimal degree of interdigitation • In normal heart, diastolic volume is the principal force that governs the strength of ventricular contraction
Frank-Starling Law (heterometric regulation) Force of contraction of myocardium Initial length of myocardial fibers Extent of preload (venous return) • Increased by • Increase in total blood volume • Increase venous tone • Increase pumping of skeletal muscle (e.g. exercise) • Atrial contraction • Decrease in intrathoracic pressure – during inspiration • Decreased by • Decrease in total blood volume • Increase in intra-pericardial pressure • Increase in intrathoracic pressure – during inspiration • Body position – sitting or standing
Pressure volume curve showing the influence of diastolic volume on the strength of ventricular contraction systolic pressure (total tension) strength of ventricular contraction pressure diastolic pressure (passive tension) volume FRANK STARLING LAW OF HEART
Significance LVF causes accumulation of blood in LV Blood supply to vital organs accumulation of blood in LV operation of Frank Starling mechanism greater LV output
Failing heart Ventricular function curves describing the relationship between preload and the systolic performance of heart Stroke volume End-diastolic volume
Factors affecting preload • Total blood volume • Venous return • Intra thoracic pressure (thoracic pump) • Cardiac pump • Pumping action of skeletal muscles • Ventricular filling(compliance) • Body position • Intra pericardial pressure
Factors affecting preload Intrathoracic pressure Thoracic pump • Inspiration: -2 mmHg -5 mmHg Diaphragm descends down VR
Factors affecting preload Cardiac pump (flow of blood in veins is towards heart) Vis-a-tergo Force from behind which drives blood forwards ( m. imp) imparted by-- Contraction of heart Elastic recoil of arterial wall Pressure of blood in veins is more than RA pressure Vis-a-fronte Force acting from front 2 components Ventricular systolic suction Ventricular diastolic suction
Factors affecting preload Role of skeletal muscle contraction Rhythmic contraction of skeletal muscles venous segments are squeezed rise of pressure forces blood towards heart venous valves prevent backflow
Factors affecting preloadVentricular compliance • Stretch imposed on cardiac muscle –determined not only by the volume of blood in the ventricles, but also by the tendency of the ventricular wall to distend or stretch in response to ventricular filling • Compliance = ∆EDV /∆EDP
Diastolic pressure volume curve in the normal and non compliant ventricle Compliance = ∆ EDV /∆EDP Normal ventricle decreased compliance End Diastolic Volume Stiff ventricle End Diastolic Pressure
HOMOMETRIC REGULATIONCardiac contractility • Intrinsic property of the cardiac cell that defines the amount of work heart can perform at a given load • Determined primarily by the availability of Ca 2+ • Attributed to interactions between contractile proteins arranged in parallel rows in the sarcomere
CARDIAC CONTRACTILITY • Indices of contractility are classified according to the phase of cardiac cycle • Isovolumic contraction phase: dP/dt dP/dt ∞ contractility ∞ initial length of the cardiac muscle • Ejection phase indices EF=SV/EDV EF is imp in predicting the prognosis of CAD • Load independent indices Time varying elastance : the ratio of ventricular pressure over volume, which varies throughout the cardiac cycle Slope of ESPVR line ∞ contractility
ESPVR is obtained by connecting all end-systolic points during a rapid decrease in preload
FACTORS AFFECTING MYOCARDIAL CONTRACTILITY Effect of changes in myocardial contractility on the Frank-Starling curve
Afterload • Load which acts on muscle after it begins to contract • Opposes muscle contraction • Systolic ventricular wall stress • Laplace law σ = P . r/2h σ = Peak systolic transmural wall tension of the ventricle P = transmural pressure across the ventricle at the end of sysole r = chamber radius at the end of diastole h = thickness
Factors affecting afterload • Wall stress • Impedance • Compliance • Effective arterial resistance • Systolic intraventricular pressure • Systemic vascular resistance • Pulmonary vascular resistance
Factors that contribute to ventricular Afterload transmural wall tension (Afterload) systolic pressure chamber radius PLEURAL PRESSURE END DIASTOLIC VOLUME Outflow impedance VASCULAR RESISTANCE VASCULAR COMPLIANCE
IMPEDANCE • Principal determinant of ventricular afterload that opposes phasic changes in pressure and flow • Most prominent in large arteries close to heart • Opposing the pulsatile output of ventricles • Influenced by Compliance- force which opposes the rate of change in flow (pulsatile flow) Resistance- force which opposes the steady flow (non pulsatile flow)
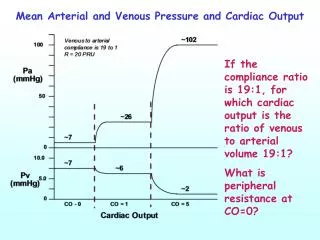
Vascular Resistance Resistance to flow in a hydraulic circuit It is expressed by the relationship between pressure gradient across the circuit (∆ P) and the rate of flow(Q) ∆ P∞ Q (Ohm’s law ) ∆ P= Q×R, where ∆ P= Pressure, Q=Flow, R=Resistance Applying Ohm’s law to CVS SVR = MAP – RAP/ CO PVR = PAP – LAP / CO Clinical implication : Shift from a low CO/ high SVR to a more favourable high CO / low SVR condition – by using vasodilators (heart failure)
Pleural pressure • Afterload (transmural) is affected by pleural pressure which acts on the outer surface of heart • -ve pleural pressure + ve pleural pressure • Opposes ventricular emptying facilitates ventricular emptying • systolic blood pressure systolic blood pressure
Respiratory variations in BP during positive pressure ventilation
Interactions between the components that regulate cardiac output and arterial pressure
Control of heart rate • Role of cardiac innervation • Role of medullary cardiovascular centres
Via sympathetic nerve cell in inermediolateral horn of spinal cord from T1-T5 spinal segment Small, myelinated preganglionic fibers Superior cardiac sympathetic ganglion Middle cardiac sympathetic ganglion Inferior cardiac sympathetic ganglion Superior cardiac sympathetic nerves Middle cardiac sympathetic nerves Inferior cardiac sympathetic nerves Cardiac innervation Sympathetic
SA node, AV node, muscles of atria & ventricles +ve inotropic effect +ve chronotropic effect +ve dromotropic effect +ve bathmotropic effect
Nucleus ambiguous Long, myelinated nerve fibres Synapse with ganglion cells near SA, AV node & atria Post-ganglionic fibres SA node, AV node, muscles of atria -ve inotropic effect -ve chronotropic effect -ve dromotropic effect -ve bathmotropic effect Parasympathetic
Medullary regulation • Medullary cardiovascular centre also known as vasomotor centre • Cardiac vagal centre
Organisation of vasomotor centre • Vasoconstrictor area – area C1 located in RVLM Contain glutaminergic neurons which excite spinal sympathetic neurons inherent tonic activity sympathetic activity pressor effect on CVS • Vasodilator area – area A1 located in CVLM Inhibit the vasoconstrictor activity of area c1
Sensory area- area A2 ( nucleus tractus solitarius ) Receives sensory signals from IX & X nerves provides reflex for controlling activity of both vasodilator and vasoconstrictor areas
VAGUS • Dorsal motor nucleus of vagus • Nucleus tractus solitarius receives afferents from baroreceptors fibres project to NA & DMNV • Nucleus Ambiguus (CARDIAC VAGAL CENTRE) • Sends vagal impulses to heart • Neurons are not tonically active
Factors affecting VMC & CVC • Baroreceptors arterial baroreceptors : carotid sinus and arch of aorta cardiac baroreceptors • Chemoreceptors : carotid and aortic bodies • Cortico hypothalamic descending pathways