Download
1 / 17
170 likes | 480 Vues
Managament of Abnormal Cervical Cytology. Assoc. Prof. Gazi YILDIRIM, M.D. Yeditepe University, Medical Faculty Dept of Ob&Gyn. Developed. Developing. Breast. 579. 471. Cervix. 91. 379. Colon/Rectum. 292. 154. Stomach. 125. 193. Lung. 175. 142. Ovary. 91. 101.

E N D
Managament of AbnormalCervicalCytology Assoc. Prof. Gazi YILDIRIM, M.D. Yeditepe University, Medical Faculty Dept of Ob&Gyn
Developed Developing Breast 579 471 Cervix 91 379 Colon/Rectum 292 154 Stomach 125 193 Lung 175 142 Ovary 91 101 Corpus uteri 114 75 Liver 34 132 Eusophagus 16 117 Non-Hodgkin Lymphoma 66 55 Leucemia 47 65 Pankreas 61 39 600 500 400 300 200 100 0 100 200 300 400 500 600 thousand Toplam 2,176,000 2,562,000 World Wide Cancer Load* *New cases in 2000 Parkin DM. Lancet Oncol. 2001;2(9):533-543.
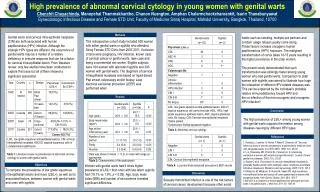
Abnormal Cytologic Findings: (The TBS, 2001) • AS cells: • ASC – US (Atypical Squamous Cell Undetermined Significance) • ASC – H (Atypical Squamous Cell cannot exclude High grade) • LSIL (Low grade Squamous Intraepitelial Lesion) • HSIL(High grade Squamous Intraepitelial Lesion) • AG cells(Atypical Glandular Cell) • AGC – NOS (Not Potherwise specified) • AGC – favorneoplasia • AIS(adenocarcinoma in situ) • InvasiveCancer
Patogenez HPV normal hücreler minimal hücresel değişiklik LGSIL(CIN I) HGSIL (CIN II-III) İnvasiv kanser
ASC-USYÖNETİMİ Sitoloji Tekrarı @ 6. ve 12. ay HPV DNA Testing LBP veya co-collection Kolposkopi Lezyon Yok ve Yetersiz Kolposkopi; ECC Sitoloji @ 6. ve 12. ay veya HPV DNA Testing @ 12. ay ASC-US Yönetimi Her İki Test (-) ≥ASC HPV (+) (LGSIL Yönetimi) HPV (-) Sitoloji Tekrarı @ 12. ay Rutin Tarama CIN YOK CIN (+) ASCCP Önerilerine Göre Yönet HPV Bilinmiyor HPV (+) ≥ASC veya HPV (+) Kolposkopi Sitoloji Tekrarı @ 12. ay Negatif Rutin Tarama
ASC-H Yönetimi Kolposkopi Sitoloji @ 6. ve 12. ay veya HPV DNA Testing @ 12. ay Kolposkopi ASC-H Yönetimi CIN 2,3 YOK CIN 2,3 ASCCP Önerilerine Göre Yönet ≥ASC veya HPV (+) Negatif Rutin Tarama
LGSIL Yönetimi Kolposkopi Non-pregnant ve Lezyon Yok ECC tercih edilir Yetersiz Kolposkopi ECC tercih edilir Yeterli Kolposkopi ve Lezyon Var ECC Yapılabilir Sitoloji @ 6. ve 12. ay veya HPV DNA Testing @ 12. ay Kolposkopi LGSIL Yönetimi* CIN 2,3 YOK CIN 2,3 ASCCP Önerilerine Göre Yönet ≥ASC veya HPV (+) Negatif *Gebe, adölesan ve postmenopozal hastalarda yönetim değişir Rutin Tarama
HGSIL Yönetimi LEEP (Adölesan ve gebeler hariç) Kolposkopi (ECC ile birlikte) Diagnostik Eksizyonel Prosedür Kolposkopi ve Sitoloji @ 6 aylık Aralarla (1 Yıl) Diagnostik Eksizyonel Prosedür HGSIL Yönetimi* CIN 2,3 YOK CIN 2,3 Yetersiz Kolposkopi Yeterli Kolposkopi Materyal Tekrarı Tanı Değişti ASCCP Önerilerine Göre Yönet Diğer Sonuçlar Negatif Sitoloji @ Her İkisi HGSIL @ Her İkisi *Gebe, adölesan ve postmenopozal hastalarda yönetim değişir Rutin Tarama
AGC Başlangıç Değerlendirme Tüm alt gruplar Atipik endom. Hc. hariç Atipik endometrial Hücreler Endometriyal ve endoservikal örnekleme Kolposkopi+ECC ve HPV testing +Endom.Bx. (yaş>35 ise) Endometrial patoloji yok Kolposkopi
New Terminology • LGL (CIN1 ±HPV) • HGL (CIN2, CIN3)
CIN’lerin Seyri CIN’lerin Seyri Östör AG, Int J Gynecol Pathol,1993
CIN 1 • 60 % Regression • 30 % Persistence • 9 % CIS • 1 % Invasive Cancer
CIN 2 • 40 % Regression • 40 % Persistence • 15 % Progression to CIS • 5 % Invasive Cancer
CIN 3 • 56 % Persistence • 33 % Regression • 12 % Invasive Cancer