PLACENTAL FUNCTION S
The placenta is a vital organ with four main functions: transport, metabolism, endocrine, and immunologic support. It plays a crucial role in fetal growth and development through an efficient maternal-fetal tissue interface, allowing for the exchange of gases, nutrients, and waste. Various mechanisms such as diffusion and active transport ensure the fetus receives essential substances. Additionally, the placenta functions as an endocrine organ, synthesizing hormones crucial for maintaining pregnancy and supporting fetal development. Understanding these functions is vital for maternal and fetal health.

PLACENTAL FUNCTION S
E N D
Presentation Transcript
PLACENTAL FUNCTIONS Associate Professor IolandaElena BLIDARU MD, PhD
PLACENTAL FUNCTIONS 4 main functions • transport • metabolism • endocrine • immunologic Placenta → essential function in the fetal growth and development.
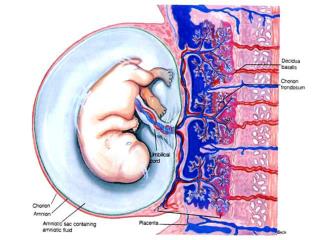
PLACENTAL FUNCTIONSThe transport function ♦ ST → the maternal - fetal tissue interface of the transcellular transfer. ♦ a functional maturity after the utero-placental circulation is established. ♦ The placenta- 2 independent circulations: the umbilical circulation+ the uterine circulation
PLACENTAL FUNCTIONSThe transport function Types of transfer across the placenta • simple diffusion (O2, CO2, anesthetic gases, water, most of the electrolytes); • facilitated transfer (glucose); • active transport (aminoacids, calcium); • receptor facilitated endocytosis (IgG, iron); • membrane disruption (uncommon); • ? restrictive diffusion (hypothetical transmembrane channels).
PLACENTAL FUNCTIONSThe transport function Facilitated diffusion Active transport mediated by proteincarriers Transfer can be modified by: - maternal nutritionel status - exercise - disease diabets mellitus hypertension alcoholism
PLACENTAL FUNCTIONSThe transport function The syncytiothrophoblast is the site of transport with substances moving from the apical membrane, across the cell wall to the basal membrane.
PLACENTAL FUNCTIONSThe transport function OXYGEN • The mechanism of O2 transport is the simple diffusion. • The O2 necessary at term is about 20ml/min→ two thirds are transferred to the fetus. • The fetus → a great capacity of maintaining the proper O2 necessary+increased possibilities to extract O2 in cases of hypoxemia. • HbF has a great affinity for O2.
PLACENTAL FUNCTIONSThe transport function CARBON DIOXIDE • The diffusion constant of CO2 is 20 times higher and facilitated by that for O2 (Haldane effect). • The placenta is highly permeable for CO2. • CO2 is present in the blood in the form of dissolved gas = carbonic acid (the most important metabolite produced by the organism),bicarbonate ion, carbonate ion and carbaminohemoglobin.
PLACENTAL FUNCTIONSThe transport function WATER TRANSFER • Exchange of water - at two main sites: - the placenta - the nonplacental chorion • Severe dehydration or over hydration → major impact on fetal homeostasis and could lead to fatal consequences.
PLACENTAL FUNCTIONSThe transport function CARBOHYDRATE TRANSFER • Glucose - the major energy substrate transported across the placenta by facilitateddiffusion via hexose transporters. • Transporter proteins for D-glucose - isolated from the plasma membrane of the microvilli of human trophoblasts. • In the glucose transfer control are involved: the maternal and fetal insulin, GRH, glucocorticoids, progesterone, estrogens, HCS (HPL) and concentration gradients.
PLACENTAL FUNCTIONSThe transport function AMINO ACID TRANSFER • Maternally derived amino acids are transferred by active transport across placenta and present in the fetal plasma in larger amounts than in the maternal plasma. • The exception → some Ig • The placental amino acids transfer → through ST
PLACENTAL FUNCTIONSThe transport function PROTEINS • Maternal IgG antibodies→ cross in significant amounts (IgG has a specific carrier that facilitates active transport). • Fc receptors(present on ST) perform the transport of Ig G through a process of pinocytosis. • The IgG1 and IgG3 subclasses are predominante (the receptor has the greatest affinity for them). • IgG1 crosses earliest in pregnancy and is the primary Ig transferred before 28 weeks.IgG3 crosses later.
PLACENTAL FUNCTIONSThe transport function LIPIDS • Neutral fats (triacylglycerols) do not cross the placenta but glycerol does. • The LDL particles are taken up by a process of endocytosis. • Cholesterol is used in progesterone synthesis. • The concentration of arachidonic acid in fetal plasma is greater than in maternal plasma (AA → a component of membranes and an eicosanoid precursor).
PLACENTAL FUNCTIONSThe transport function VITAMINS AND MINERALS • The fat-soluble vitamins are transported as lipoproteins complexes. • The water-soluble vitamins & Ca, Mgactive transport. • The placental transfer of Ca→ influenced by: metabolites of vitamin D parathormone prolactin calcitonin • The placental transfer of FE++→ receptor mediated endocytosis.
PLACENTAL FUNCTIONSEndocrine function The placenta is a major endocrine organ. The placenta synthesizes hormones and cytokines that have major influences on ovarian, uterine, mammary and fetal physiology. Fetal, placental & maternal compartments form an integrated hormonal unit The feto-placental-maternal (FPM) unit creates the Endocrine Environment that maintains and drives the processes of pregnancy and pre-natal development.
PLACENTAL FUNCTIONSEndocrine function Steroid Hormones: 1- Estrogens 2- Progesterone Protein hormones: 1- Human chorionic gonadotrophin (hCG) 2- Human placental lactogen (hPL) 3- Human chorionic thyrotrophin (hCT) 4- Hypothalamic and pituitary like hormones 5- Others: inhibin, relaxin and beta endorphins.
Estrogens in ovary The two-cell-two gonadotropin principle of ovarian steroid hormone production. 1. During the follicular phase - luteinizing hormone (LH) controls theca cell production of androstenedione, which diffuses into the adjacent granulosa cells and acts as precursor for E2 biosynthesis. The capacity for the granulosa cell to convert androstenedione to E2 is controlled by follicle-stimulating hormone (FSH).
Estrogens in ovary 2. After ovulation, the corpus luteum forms and both theca-lutein and granulosa-lutein cells respond to LH. The theca-lutein cells continue to produce androstenedione, whereas granulosa-lutein cells greatly increase their capacity to produce P and to convert androstenedione to E2. If pregnancy occurs, the production of hCG by the placenta rescues the corpus luteum.
PLACENTAL FUNCTIONSEndocrine function Estrogens • Synthesized by syncytiotrophoblast from their precursors: • dehydroepiandrosteronesulphate (DHES) • 16 α -hydroxydehydroepiandrosteronesulphate (16 α - OH- DHES). 90% of 16α - OH – DHES (dehydroepiandrosteronesulphate) is derived from fetal origin (hydroxylation of DHES in the fetal liver). 10% 16α - OH - DHES is derived from the mother (by the same way). • It is transformed in the placenta intoestradiol - 17b (E2).
PLACENTAL FUNCTIONSEndocrine function Estrogens • Maternal urinary and serum estriol important index for fetal wellbeing as its synthesis depends mainly on the integrity of the fetal adrenal and liver as well as the placenta. (feto- placental unit) • Estrogens are excreted (90%) in the maternal urine as estriol (E3). • Urinary estriol increases as pregnancy advances to reach 10-14 mg / 24 hours in late pregnancy.
Schematic presentation of the biosynthesis of estrogens in the human placenta • Dehydroepiandrosterone sulfate (DHEA-S), secreted by the fetal adrenal glands, is converted to 16 -hydroxydehydroepiandrosterone sulfate (16 OHDHEA-S) in the fetal liver. • These steroids, DHEA-S and 16 OHDHEA-S, are converted in the placenta to estrogens, that is, 17 -estradiol (E2) and estriol (E3). • Near term, half of E2 is derived from fetal adrenal DHEA-S and half from maternal DHEA-S. On the other hand, 90 percent of E3 in the placenta arises from fetal 16 OHDHEA-S and only 10 percent from all other sources.
PLACENTAL FUNCTIONSEndocrine function Principal biological effects of placental estrogens • stimulate growth of the myometrium • antagonize the myometrial-suppressing activity of P • stimulate mammary gland development • control over the synthesis and secretion of some proteins during the first trimester • the cervical ripening • in late gestation induces:myometrialoxytocin receptors, myometrial gap junction stimulation, stimulation of the synthesis and release of PG and contractile proteins, stimulationover the membrane permeability and on the myometrial electric activity (preparing the uterus for parturition).
PLACENTAL FUNCTIONSEndocrine function Progesterone • It is synthesized by syncytiotrophoblast from the maternal cholesterol. • Estrogens, PG, some growth factors increase P synthesis. • Excreted in maternal urine as pregnandiol.
PLACENTAL FUNCTIONSEndocrine function Progesterone Roles of P in maintaining pregnancy: • a local immune protection role; • a role in the development of the placental tissue and in the increase of placental vasculature; • inhibition of myometrial contractility.
Changes in concentrations of progesterone and estrogens in the maternal serum of humans through gestation.
PLACENTAL FUNCTIONSEndocrine function Human chorionic gonadotrophin(hCG) It is a glycoprotein produced by the syncytiotrophoblast. It supports the corpus luteum in the first 10 weeks of pregnancy to produce E2 and P until the syncytiotrophoblast can produce them. HCG molecule → composed of 2 subunits: a. Alpha subunit - similar to FSH, LH, TSH. b. Beta subunit - specific to hCG.
PLACENTAL FUNCTIONSEndocrine function Human chorionic gonadotrophin (hCG) • HCG - determined in urine, beginning with the 45th day of gestation. • In the 5th-6th weeks peak values indicate a normal pregnancy (in evolution). low values→ectopic pregnancy → interruption of intrauterine pregnancy • HCG rises sharply after implantation, reaches a peak of 100.000 mIU/ml about the 60-th day of pregnancy (w 5-6). • HCG falls sharply by the day 100 and is maintained at this level until term
PLACENTAL FUNCTIONSEndocrine function Human placental lactogen (HPL) (chorionic somatomammotropin) It is a polypeptide hormone produced by the SC. The actions of hPL a. Lipolysis: increasing free fatty acids - provide a source of energy b. Inhibition of gluconeogenesis: spare both glucose and protein - the anti-insulin effect of hPL. c. Somatotrophic: fetal growth promotion. d. Mammotropic and lactogenic effect.
PLACENTAL FUNCTIONSEndocrine function Human placental lactogen (HPL) (chorionic somatomammotropin) HPL - detected by the 5-6th week of pregnancy, rises steadily until the 36th week to be 6 mg/ml. HPL values - one of the best criteria to watch the evolution of pregnancy in the third trimester. Low levels - fetal distress, IUGR, intrauterine death, chronic placental insufficiency (serial measurements). screening test
PLACENTAL FUNCTIONSEndocrine function Hypothalamic and pituitary - like hormones • Gonadotropin releasing hormone (GnRH) • Corticotropin releasing hormone (CRH) • Growth hormone – releasing hormone (GH) • Proopiomelanocortin – derived peptides: ACTH, Melanocyte stimulating hormone, (MSH), Beta endorphins and lipotrophins • Neurohypophyseal peptides: OXT, Argininevasopressine (AVP) • Growth factors: EGF, insulin and insulin-like growth factors (IGF I, IGF II) • Inhibin, Activin, Relaxin
SRAA in pregnancy • RENIN, ANGIOTENSIN II, AND PLASMA VOLUME • The renin-angiotensin-aldosterone axis is intimately involved in renal control of blood pressure via sodium and water balance. • Renin is produced by both the maternal kidney and the placenta • Increased renin substrate = angiotensinogen is produced by both maternal and fetal liver.
SRAA in pregnancy • Nulliparas who remained normotensive became and stayed refractory to the pressor effects of infused angiotensin II. • Conversely, those who ultimately became hypertensive developed, but then lost, this refractoriness. The vascular responsiveness to angiotensin II is progesterone related.
PLACENTAL FUNCTIONSPlacental immunologicalphenomena • The placenta functions as an immunological “barrier” between the mother and the fetus. • Trophoblast is the contact zone between the maternal tissues and embryo-fetal structures. • The trophoblast membranes are not immunologically inert. • The maternal immune system facilitates the fetal semiallograft.
PLACENTAL FUNCTIONSPLACENTAL IMMUNOLOGICALPHENOMENA Trophoblast antigens They may be grouped into 3 categories: • major histocompatibility complex antigens (MHC) = HLA • antigens with suspected functions (trophoblast — lymphocyte cross-reactive antigens — TLX, transferrin, the major basic protein) • antigens with unknown functions.
PLACENTAL FUNCTIONSPLACENTAL IMMUNOLOGICALPHENOMENA The immunological processes in pregnancy is related to the presence of cytokinesin the MPF unit. interleukins, α and β TNF and interferons The placenta may have an immunoregulatory role as demonstrated by the release of factors that suppress lymphocyte activation. Cytokines → major mediator in the immunological phenomena of pregnancy.
IMMUNOGENICITY OF THE TROPHOBLASTS • The placenta - considered immunologically inert and therefore unable to create a maternal immune response. • MHC class I and II antigens are absent from villous trophoblasts, which appear to be immunologically inert at all stages of gestation. • Invasive extravillous cytotrophoblasts do express MHC class I molecules: HLA-C, HLA-E and HLA-G.
UTERINE NATURAL KILLER CELLS • Normal implantation depends on controlled trophoblastic invasion of maternal decidua and spiral arteries. Such invasion must proceed far enough to provide for normal fetal growth and development, but there must be a mechanism for regulating its depth. • The uterine decidual natural killer cells (uNK cells) combined with the unique expression of the 3 specific HLA class I genes in extravillous cytotrophoblasts act in concert to permit and subsequently limit trophoblast invasion. • These uNK cells secrete large amounts of TH2 - cytokines.