Download
1 / 32
370 likes | 843 Vues
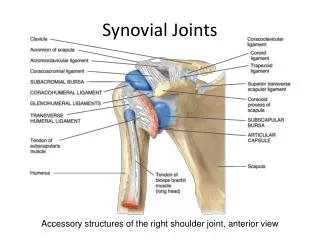
Synovium, non-synovial joints, and bone physiology and diseases. Lecture 8 Tuesday, January 30, 2007 Ref. Wheater’s Functional Histology Chapter 10, Ross and Pawlina Chapter 8, Chapter 6 Medical Physiology p. 1088-1090 Basic Pathology p. 756-761. Synovium.

E N D
Synovium, non-synovial joints, and bone physiology and diseases Lecture 8 Tuesday, January 30, 2007 Ref. Wheater’s Functional Histology Chapter 10, Ross and Pawlina Chapter 8, Chapter 6 Medical Physiology p. 1088-1090 Basic Pathology p. 756-761
Synovium • Specialized connective tissue not epithelium • Surface is a discontinuous layer up to 4 cells deep. • Lining cells are not connected by junctional complexes. • Lining cells are not resting on basement membrane. • Contains vessels and nerves. • May be loose (areolar), fibrous, adipose, folded, or villi. • Two synovial cell types • Type A synoviocytes - majority, plump, have numerous lysosomes • Type B synoviocytes - fibroblast-like, secretory
Synovium WFH 10.29Plump cells are type A; fibroblast like cells are type B
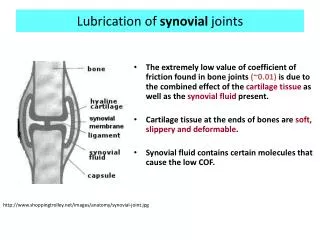
Synovial Fluid • A specialized form of ECM • Hyaluronic acid, glycoproteins, • Secreted by type B synoviocytes • Fluid component is a transudate from capillaries • Diffusion of oxygen, nutrients and metabolites between blood and synovial fluid. • Viscous, transparent • Few leukocytes (<100/µl)
Non-synovial joints • Dense fibrous • Syndesmoses e.g. sutures of skull • Become synostoses after replacement by bone. • Hyaline cartilage • Synchondrosis or primary cartilaginous joint • In adult human- vertebrocostal ribs with the sternum • Fibrocartilage • Symphyses or secondary cartilaginous joints • Apposing bones are covered by hyaline cartilage and directly connected by fibrocartilage. • e.g. pubic symphysis and intervertebral disks
Intervertebral joints WFH 10.29Two types: fibrocartilage between bodies of vertebrae andsynovial between vertebral arches
Intervertebral disc • Annulus fibrosus • Concentric rings of fibrocartilage surround a central cavity • Nucleus pulposus • Viscous fluid supporting tissue that is a remnant of the notochord. (Notochord is derived from mesoblast of embryo and defines the primitive axis of the body) • ECM consists of ground substance only • Cells suspended in fluid are physaliphorous cells. • Acts as a shock absorber.
Disc herniation • Annulus fibrosis weakens with age. • Compression may cause herniation of the nucleus pulposus. • Weakest ligaments are posterior lateral. • Extruded material puts pressure on spinal cord or spinal nerve root. • Herniations are usually in the lumbar or cervical areas.
Bone physiology • Remodeling is continual process • 80% total bone is compact • 20% is trabecular-higher fractional rate of turnover • Osteocytic osteolysis • Transfer of Ca++ from interior to surface via interconnected osteocytes • Nutritional requirements • Vitamin C, vitamin D, Calcium
Normal bone formation/resorption • Osteoblast • Makes osteoid • Influences osteoclast differentiation via • RANKL (also on stromal cells and T cells) interaction with RANK on precursor monocytes • Secretion of M-CSF • Makes osteoprotegerin that binds to RANK ligand preventing RANK ligand from stimulating osteoclasts • Has receptors for hormones and cytokines, IL-1, TNFa and secretes mediators that influence osteoclast activity • Factors released from the digested bone matrix (cytokines, growth factors) trigger osteoblast to deposit an equivalent amount of new bone.
Bone Pathology Overview • Abnormalities of quality/quantity of bone • Osteoporosis, osteopetrosis, osteomalacia • Osteogenesis imperfecta • Paget’s disease • Infection • Osteomyelitis (bacterial, fungal) • Neoplasia • Primary malignant, benign, or metastatic
Osteoporosis • Relative excess of osteoclastic function. • Net loss of bone. • Trabecular bone is more active metabolically and lost more rapidly. • Increased incidence of fractures • Forearm, vertebrae, and hip
Types of osteoporosis • Involutional-primary, senile • Disuse • Immobilization (local or weightlessness) • Secondary • Drug related e.g. corticosteroids • Corticosteroids increase the production of RANK ligand but decrease the production of osteoprotegerin-- bone loss • Endocrine • Gastrointestinal • Neoplasia
Involutional osteoporosis • Most common • Affects both men and women • Peak bone mass is reached in early adulthood and depends on • Genetic factors (vitamin D receptor) • State of nutrition • Level of physical activity • Hormonal status
Estrogen’s effects on bone • Estrogen inhibits secretion of IL-1, IL-6, and TNFa • Estrogen stimulates production of TGFb • TGFb increases apoptosis of osteoclasts • Net effect of estrogen treatment is to reduce or arrest bone loss • Other inhibitors of osteoclasts are bisphosphonates
Osteopetrosis • Rare, hereditary, autosomal recessive or dominant • Stone-like bone, solid on radiographs • Actually brittle, fractures easily • Pressure on nerves • Optic nerve atrophy • Caused by osteoclast dysfunction • Lack of bone marrow • Increased infections, lack of precursors for osteoclasts
Rickets and osteomalacia • Defect in matrix mineralization • Often due to vitamin D deficiency • Rickets in children • Weakness and bowing of weight-bearing bones • Defects in teeth • Hypocalcemia • Osteomalacia in adults • Vulnerable to fractures, especially vertebrae and femoral neck
Actions of vitamin D • Increase calcium absorption from GI tract • Increase reabsorption of calcium in kidneys • Stimulate synthetic activity of osteoblasts • secrete osteocalcin which binds Ca++ • secrete M-CSF which causes proliferation of osteoclast precursors • Required for mineralization of matrix • With other hormones controls calcium metabolism
Osteogenesis Imperfecta • A group of diseases due to deficiencies in synthesis of type I collagen • Autosomal dominant or recessive • In some forms mutant allele acts as a dominant negative • Fragile, brittle bones • Joint laxity • Eyes- blue sclera • Teeth • 4 major types-most common is autosomal dominant • Variable signs from mild to lethal in utero • suspicion of child abuse
Bone disease associated with hyperparathyroidism • Excess parathyroid hormone activates osteoclasts • Primary • Rare, tumor of parathyroid gland • Secondary • Renal disease factors in addition to high PTH: • Decreased production of vitamin D. • Decreased calcium absorption from gut. • Metabolic acidosis. • Paraneoplastic syndrome • Nutritional • Lack of calcium in diet
Paget Disease (Osteitis Deformans) • Etiology unknown, possibly paramyxovirus • Higher incidence in whites in England, France, Australia, New Zealand, USA • Rare in Scandinavia, China, Japan, and Africa • Affects middle-aged or older adults • Often asymptomatic • 3 phases (repeating and overlapping) • Osteolytic, haphazard, inappropriate osteoclastic activity • Mixed- osteolysis and rapid bone formation • Osteosclerotic • Net effect more bone (woven bone), but weaker • Pain and predisposition to fractures and tumors
Paget Disease Mosaic pattern PBD 28-13BP 21-5New bone is woven bone--lacks normal lamellar architecture.
Osteomyelitis (infection of bone and marrow) • Acute osteomyelitis • Pyogenic bacteria • 80-90% are Staphylococcus aureus • Pneumococci and gram negative organisms • Mixed bacteria -- common after trauma • Route • Hematogenous - more common in infants and young children • Penetrating injury- compound or open fracture • Extension from adjacent infection • Sequestrum (necrotic bone) • complicates healing • Acts as a foreign body and haven for microorganisms
Chronic osteomyelitis with sequestrum BP 21-3PBD 28-19Often draining tracts open onto the skin.