Knee Ligament Injuries
470 likes | 1.35k Vues
Knee Ligament Injuries. Overview. Ligament Anatomy Biomechanics Ligament Specific Epidemiology Classification Clinical exam Imaging Tx. Ligament Anatomy. Type 1 collagen (70%) Elastin Extracellular matrix Hierarchical structure Fibrils > fibres >subfascicular unit >fasciculus

Knee Ligament Injuries
E N D
Presentation Transcript
Overview • Ligament Anatomy • Biomechanics • Ligament Specific • Epidemiology • Classification • Clinical exam • Imaging • Tx
Ligament Anatomy • Type 1 collagen (70%) • Elastin • Extracellular matrix • Hierarchical structure • Fibrils > fibres >subfascicular unit >fasciculus • Longitudinal fasciculi (MCL, LCL) • Helical fasciculi (ACL, PCL)
Anatomic Features • Bonding • Crimping • Random collagen alignment • Complex blood supply • Diffusion from synovium • Proprioception and nociception
Biomechanics • Laxity • Stiffness • Strength • Viscoelastic behavior (creep, stress relaxation, hysteresis) • Dynamic properties
Ligament healing • Immobilization • Loading dramatically affects recovery of normal mechanical properties • Decrease strength • Insertion site vs. midsubstance • Exercise • Favourable effect
Epidemiology • Increasing incidence • Combined injuries common • Females > males • Conditioned vs. unconditioned
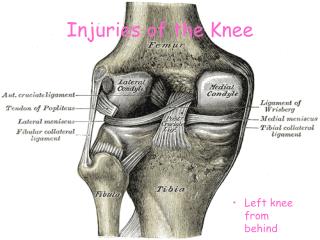
ACL Anatomy • Intracapsular • Extrasynovial • Varied blood supply • FAMPLE • Origin / Insertion
ACL Function • Limit anterior displacement • 20 restraint rotation • 20 restraint varus / valgus in extension
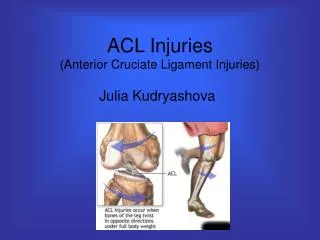
Mechanism / Hx • Usually noncontact • Change direction • Stop / jump • Audible “pop” • Instability • Swelling
General Ligament Exam • Difficult acutely • Early exam beneficial • Pt. relaxed • Displacement • Endpoint quality • Compare
ACL Exam • Lachman – best • Pivot Shift – diagnostic • Anterior drawer – chronic tear • Associated injuries
ACL Imaging • XRAY • R/O # • ACL avulsion • Segond # • Arthrography - poor • Arthroscopy - gold standard
ACL MRI • 95% accurate • Low signal intensity • Saggital view • Acute injury high signal intensity on T2 image • Bone bruising
ACL Tx • Pt selection • Operative vs. Non-operative • Demand level • Modify lifestyle • ACL dependent • Other lesions
Non-operative • Acutely – splint & crutches • Early active ROM • Closed chain WB to strengthen • Avoid high risk • Functional bracing controversial
Operative • Pt selection • High demand • Young • Good ROM • Open vs. endosopic • Learning curve
Graft • Auto vs. allo • Collagen lattice • Resorption – revascularization – restructuring • Bone-patellar tendon-bone • Semitendinosus/gracilis • tensioning
Rehab • Closed kinetic chain strengthening • Acutely fixation weak • Graft weakest 6-12 wks • Outcome • >90% stable 3-5 yrs
MCL Anatomy • Origin – femoral condyle • Insertion – 4cm below joint line • + posterior obl. Lig. • + middle capsular ligament • Parallel collagen
MCL • Most common isolated ligament injury • Valgus force • Post. Obl. Lig. damage with rotn. injury • Associated ACL common
MCL exam • Valgus force • Flex. 300 – isolated • Extension • Assoc. POL,ACL,PCL • 5-8 mm difference significant • Swelling • Hemarthrosis vs. soft tissue
MCL Tx • Non-surgical • RICE • Bracing • Strengthening • Functional brace
MCL Classification / Tx • Grade 1 : 1-5 mm • Symptomatic Tx • Grade 2 : 6–10 mm • Hinge brace 2-3 wks • Grade 3 : 11-15 mm • Hinge brace 3-4 wks • Physio
PCL Injury • 1.5 x ACL strength • 5% all knee lig. inj. • 10 restraint post. translation tibia • Forced flexion • Dashboard • Associated injuries
PCL • Pain • Usually stable • Posterior subluxation • Medial & patellofemoral OA
PCL exam • Posterior drawer test –best • Grade I - III • Quadriceps active test • Post sag sign
Non-operative • Aggressive rehab • Focus quadriceps • No support for bracing • closed kinetic chain • Open kinetic chain extension avoided • 90% quads strength prior to normal athletics
PCL Tx • Repair : • Associated posterolateral corner • Associated ACL / MCL • Grade 3 Drawer test • Bony avulsion • 20% athletes with isolated injury require repair
Operative Repair • Require good ROM pre-op • Graft > 40mm • No good rehab protocol
Posterolateral Complex • Combination of Structures • ITB • biceps femoris • fibular collateral • Popliteus complex • Capsule • etc
Posterolateral corner • Usually assoc with: • PCL • Knee dislocation • Rarely ACL • Instability esp descending inclines • Peroneal N. inj. 10% • pain
Biomechanical • Increased: • External tibial rotation • Varus rotation • Posterior tibial translation
Exam • Swelling / bruising • Gait : Varus thrust • AP translation > 300 than 900 • Best tests: • Varus stress opening > 300 than 00 • Prone external rotation test • Other tests
Operative • 10 Repair • Acute injury • Bony avulsion • Reconstruction • Biceps tenodesis / arcuate lig advancement : mixed results • Graft - results pending • Varus malalignment - HTO
Conclusion • Common injuries • Easily missed • Large area • Ongoing research