Download
1 / 21
270 likes | 492 Vues
Organization of the Motor System. Motor Organization – The Big Picture. There are several systems that enable smooth and exact purposeful movements. The corticospinal and corticobulbar systems are the

E N D
Organization of the Motor System
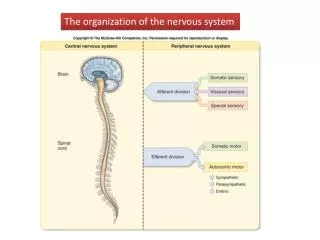
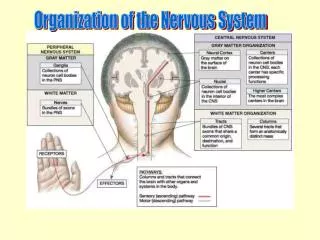
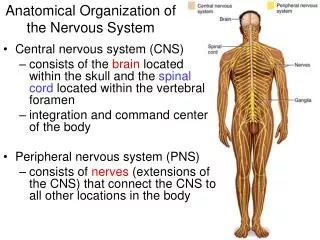
Motor Organization – The Big Picture There are several systems that enable smooth and exact purposeful movements. The corticospinaland corticobulbarsystems are the most important voluntary motor systems. The motor signals generated in the cerebral cortex are relatively coarse and need modulation, however, as facilitated by the basal ganglia and the cerebellum. Other voluntarily regulated motor pathways are the rubrospinal and the reticulospinaltracts. The two vestibulospinaltracts receive sensory input from the vestibular nuclei but are not directly influenced by the cerebral cortex. They are thus largely involuntary motor pathways. The motor system receives also somatosensoryinput via the muscle spindles, the dorsal column/medial lemniscus pathways, the somatosensory cortex, the anterolaleral system (ALS), and thereticulospinaltracts.
Motor Pathways The lateral corticospinal tract is a long motor pathway between the cortex and the spinal cord,several long motor Pathways also start in the brainstem and end in the spinal cord. Start of the Motor Pathways
End of the Motor Pathways The descending motor tracts (at spinal levels) are subdivided into the ventromedial (also called anteromedial) and the lateral pathways. The ventromedial tracts are: · Pontine (medial) reticulospinal · Lateral vestubulospinal · Medial vestibulospinal The lateral tracts are: · Lateral corticospinal · Rubrospinal · Medullary (lateral) reticulospinal
Location of Motor Neurons in Relation to Function In the ventral horn of the spinal cord, flexor and adductor neurons lie dorsal to the extensor and abductor neurons. Cells for distal muscles lie laterally to those for trunk structures (i.e., proximal muscles). Relations between Motor Neurons and Spinal Pathways Lateral Pathways are Biased for Flexion of the Limbs Medial Pathways are Biased for Extension of the Limbs
Corticospinal Tract Initiation and Control of Motor Activity The corticospinal tract is the most important motor pathway. Prefrontal areas (motor planning) project to the premotor cortex (production of motor programs), which then communicates with the primary motor cortex (execution of excitatory drive for motor activity). (Brodmann’s area 4) Brodmann’s area 4 is often called the primary motor cortex. Premotor and Supplementary Cortices (Brodmann’s area 6)
Homunculus Each distinct area in the primary motor cortex is responsible for the motor control of a particular part of the body. The representation of the body that can be functionally mapped against such a region is called a “homunculus.”
Predominant Role of the Lateral CorticospinalTract The main function of the lateral corticospinal tract is voluntary contraction of distal flexor muscles of the limbs (e.g., it is thus integral to reaching and walking). Sensory input from the periphery is processed by the cortex, which constantly modifies the signals transmitted by this tract. Inputs into the cortex from the basal ganglia and cerebellum via the thalamus also always modulate lateral corticospinaloutput.
Start of Lateral Corticospinal Tract The origin of the corticospinal tract is the pyramidal cell bodies located in layer 5 of the precentralgyrusand anterior paracentral lobule. End of Lateral Corticospinal Tract The end of the corticospinal tract is the contralateral anterior horn of the spinal cord, where the axons of the upper motor neurons synapse with alpha and gamma lower motor neurons
Route of Corticospinal Tract · corona radiata · internal capsule (posterior limb) · cruscerebri · basilar pons · corticospinal tracts in spinal cord · synapses on alpha and gamma neurons in spinal anterior horn
Approximately 90% of the fibers from motor cortex cross over at the pyramidal decussation(caudal medulla) to form the lateral corticospinal tract. Ten percent remain ipsilateral to enter the cord as the ventral (anterior) corticospinal tract. Damage to the lateral corticospinal tract rostral to the pyramidal decussation produces contralateralhemiparesis. Damage to the lateral corticospinal tract caudal to the decussation produces ipsilateralhemiparesisat and below the lesion.
Upper Motor Neurons · Upper motor neurons forming the corticospinal and corticobulbar tracts arise from cell bodies located in layer 5 of the primary motor cortex. The corticospinal fibers project through the corona radiata, internal capsule, cruscerebri, basal pons, and pyramid, entering the spinal cord to terminate (largely) in the contralateral anterior (ventral) horn. Direct or indirect excitatory synaptic contact is made with a second order motor neuron (lower motor neuron). Lower Motor Neurons · The cell bodies of the lower motor neurons dwell in the ventral horn of the spinal cord (receiving inputs from corticospinal fibers) and the motor nuclei of the brainstem (receiving inputs from corticobulbar fibers). They send axons directly to skeletal muscle fibers to effect muscular contractions.
Lower Motor Neuron Lesion – Symptoms occur ipsilateral to site of the lesion -- Flaccid paralysis (loss of movement) – Hyporeflexia/areflexia(due to interruption of the efferent (motor) limb of the sensory-motor reflex arcs. – fasciculations Wasting of muscles, -- atonia or hypotonia(muscle tone reflects sustained partial contraction of muscular fibers and depends directly on the monosynaptic reflex arc that connects the muscle spindles to the lower motor neurons) Examples of diseases that involve LMN syndrome are: · Amyotrophic lateral sclerosis · Peripheral nerve damage (traumatic)
Diseases of the Lower Motor Neuron Amyotrophic Lateral Sclerosis (Lou Gehrig’s Disease) It is a progressive neuromuscular disease that initially affects and later destroys lower motor neurons and eventually also parts of the pyramidal tract and the precentralgyrus(and the anterior portion of the paracentral lobule) ALS patients usually develop muscle weakness and difficulty speaking and/or swallowing. Sphincter control, sensory function, intellectual ability, and skin integrity are not commonly affected.
Upper Motor Neuron Lesion – Lesion above decussation: symptoms contrlateral to the lesion – Lesion below the decussation: symptoms ipsilateral to the lesion – Hyperreflexia – Extensor plantar response – First flaccid paralysis, later spastic paralysis – No wasting of muscles (because 2nd motor neuron is not impaired)
Paraplegia Paraplegia occurs after a bilateral spinal cord injury. In most cases, a traumatic event impairs the cells within the spinal cord or cuts or crushes the fibers of the long tracts (through bruising, compression, or laceration). The symptoms of paraplegia are: · flaccid paralysis below the level of the lesion (i.e., related to spinal shock), followed days-to-weeks later by spasticity. · increased deep tendon reflexes and clonus. · extensor plantar response (Babinski sign). · early retention of urine with painless distension of the bladder and overflow, as pressure overcomes the reflex closure of bladder sphincters. Reflexive emptying of bladder accompanies the lifting of spinal shock. · paraplegia in flexion (physiotherapy is warranted). · loss of all somatosensation from below the lesion.
Other Motor Pathways 1. Rubrospinal Tract (Flexor Muscles) Start: Red nucleus in midbrain End: Alpha and gamma motor neurons in the anterior horn of the spinal cord. Function- stimulation of flexors of upper limb. 2. Medullary (Lateral) Reticulospinal Tract (Flexor Muscles) -originates in the nuclei of medulla and ends in anterior horn of spinal cord. - Most fibers of the medullary reticulospinal pathway facilitate contraction of flexor muscles of the limbs.
3. Pontine (Medial) Reticulospinal Tract (Extensor Muscles) • originates in the nuclei of medulla and ends in anterior horn of spinal cord. • End: anterior horn of the spinal cord. • Most fibers in this pathway facilitate • contraction of extensor muscles of the limbs. 4. Lateral Vestibulospinal Tract (Extensor Muscles) Start: Lateral vestibular nucleus. End: anterior horn of the spinal cord 5. Medial Vestibulospinal Tract (Extensor Muscles)-simillar to lateral vestibulospinal tract.
Decorticate Posturing A lesion rostral to the red nucleus that impairs corticospinal, produces decorticate posturing. After a noxious stimulus or spontaneously, the affected patient will flex the upper limbs and extend the lower limbs. corticospinal tract interrupted – mainly flexion impaired • rubrospinal tract intact – flexion of the arms • ·medullaryreticulospinal tract intact – flexion of extremities • ·pontinereticulospinal tract intact – extension of extremities • ·vestibulospinal tracts intact – extension of extremities • Arms • In the arms, the flexor input of the rubrospinal tract is still intact. Hence, there is strong flexor innervation, which is much greater than the extensor input of pontinereticulospinal and vestibulospinal tracts. • Legs • For the lower limbs rubrospinal tract has almost no impact, hence the extensor innervation is much more relevant, so the lower limbs are extended.
Decerebrate Posturing A lesion below the red nucleus that impairs the corticospinal, corticobulbar, and rubrospinal Fibers produces decerebrate posturing. After a noxious stimulus or spontaneously, the patient will extend the upper and lower limbs. · corticospinal tract interrupted – mainly flexion impaired · corticobulbar tract interrupted – paralysis of motor CNs · rubrospinal tract interrupted – no flexion of arms · medullaryreticulospinal tract intact – flexion of extremities · pontinereticulospinal tract intact – extension of extremities · vestibulospinal tracts intact – extension of extremities In the upper and lower limbs, there is flexor input from only the medullary reticulospinal tract, which is overruled by the extensor innervation of the pontinereticulospinal and vestibulospinal tracts.