Download
1 / 21
570 likes | 4.84k Vues
Chapter 8 for 12 Lead Training -The 15 Lead ECG-. Ontario Base Hospital Group Education Subcommittee 2008. TIME IS MUSCLE. The 15 Lead ECG. REVIEWERS/CONTRIBUTORS Neil Freckleton, AEMCA, ACP Hamilton Base Hospital Jim Scott, AEMCA, PCP Sault Area Hospital Ed Ouston, AEMCA, ACP

E N D
Chapter 8 for 12 Lead Training-The 15 Lead ECG- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE
The 15 Lead ECG REVIEWERS/CONTRIBUTORS Neil Freckleton, AEMCA, ACP Hamilton Base Hospital Jim Scott, AEMCA, PCP Sault Area Hospital Ed Ouston, AEMCA, ACP Ottawa Base Hospital Laura McCleary, AEMCA, ACP SOCPC Tim Dodd, AEMCA, ACP Hamilton Base Hospital Dr. Rick Verbeek, Medical Director SOCPC AUTHOR Greg Soto, BEd, BA, ACP Niagara Base Hospital 2008 Ontario Base Hospital Group
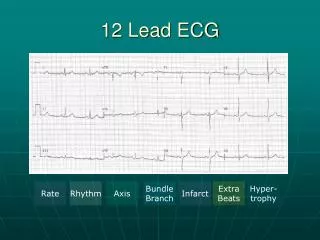
Chapter 8 - Objectives • Describe the benefits of acquiring a 15-lead ECG • Describe the proper lead placement for Leads V4R, V8, and V9 • Describe the hemodynamic problems associated with a right ventricular infarction • List 3 clinical signs of RVI • On a 15-lead ECG, recognize ECG changes for a posterior and right ventricular MI
Why a 15-Lead ECG? • Used when a patient has an Inferior STEMI or suspected Posterior STEMI (reciprocal changes with ST depression in V1/V2) • Can confirm Posterior MI (usually associated with an Inferior MI • Can suggest RVMI which is a larger and more complicated Inferior MI
Acquiring the 15-Lead (V4R) • Run standard 12-lead • Lead V4R: 5th IC space midclavicular on right side • Same as left side V4 • Attach V4 wire to the V4R position
Acquiring a 15-Lead (V8, V9) • Posterior leads • V8: 5th IC space midscapular line • V9 goes between V8 and the spine • Place Lead V5 wire on V8 and V6 wire on V9 • Acquire the second 12-lead • Re-label the new leads
Right Ventricular Infarction • RV gets blood supply from the RCA • Up to 50% of inferior MI will have RVI • RV is preload dependant for Cardiac Output • Nitrates cause preload reduction; thus use nitrates with extreme caution • Hypotension in RVMI often responds well to IV fluid bolus (increase in preload) • May require 1 liter or more IV fluid bolus for hypotension
Clinical Signs of RVI The TRIAD: • Jugular vein distention (JVD) • Hypotension, either presenting or following nitro administration • Clear lung sounds
Right Coronary Artery • Inferior wall of LV • Right ventricle • Posterior LV • Posterior fascicle of LBB • SA and AV node • 2nd deg I common
Indications - 15 Lead ECG • Any Inferior AMI (but especially accompanied by ST-depression in V1 to V3) • ST-depression in V1 – V3 on its own in symptomatic ACS patient
START QUIT Well Done! Education Subcommittee