Download
1 / 29
330 likes | 1.54k Vues
Crush Injuries and Rhabdomyolysis Dr.M.Mortazavi Nephrologist. INTRODUCTION. Rhabdomyolysis is a syndrome characterized by muscle necrosis and the release of intracellular muscle constituents into the circulation.

E N D
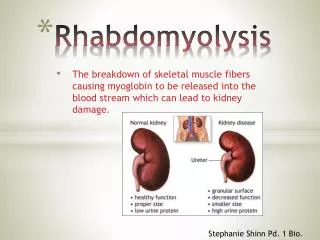
INTRODUCTION • Rhabdomyolysis is a syndrome characterized by muscle necrosis and the release of intracellular muscle constituents into the circulation. • The severity of illness ranges from asymptomatic elevations in serum muscle enzymes to life-threatening cases associated with extreme enzyme elevations, electrolyte imbalances, and acute renal failure
“Crush syndrome” first recorded in bombing of London during WWII: 5 people who were crushed presented in shock with swollen extremities, dark urine. • Later died from renal failure. • 5-35% of patients with rhabdomyolysis develop ARF • mortality is 3-50%
Cause of Rhabdomyolysis • Traumatic muscle injury • Drugs and toxins • Infections • Genetic disorders • Excessive muscle activity • Ischemia • Electrolyte and endocrine • Immunologic disease
Myocyte Injury Tolerable-no permanent histological changes Muscle necrosis Hours of ischemia 0 2 4 6 Irreversible anatomic and functional changes
Cell Ion Physiology intracellular extracellular
Pathogenesis of Myocyte Injury Ca++ compression Protease activation Membrane degradation Nuclease activation Lipid peroxidation ischemia Influx of Ca++, Na+ and fluids Attraction of PMN’s Decreased ATP production cell lysis More Ca++ influx
Pathophysiology of ARF CONTRIBUTORS: • Dehydration (hypovolemia) • Aciduria • Renal vasoconstriction • Cast formation • Heme-induced toxicity to tubule cells Not reabsorbed Binds Tamm-Horsfell proteins Myoglobin – 1-3% of wet mm weight
Rhabdomyolysis Myoglobinemia Endotoxin cascade 3,rd spacing NO scavenging Myoglobinuria Volume depletion Acidemia Proxmial tubule Fe loading Aciduria Renal hypoperfusion/ Ischemia Cast formation Luminal stasis Synergistic tubular damage ARF ATN
CLINICAL MANIFESTATIONS AND DIAGNOSIS • The classic presentation of rhabdomyolysis includes myalgias, red to brown urine due to myoglobinuria, and elevated serum muscle enzymes (including creatine kinase)
When to Suspect Rhabdo • Occurs in up to 85% of patients with traumatic injuries. • Those with severe injury who develop rhabdomyolysis-induced renal failure have a 20% mortality rate • Multiple orthopedic injuries • Crush injury to any part of the body (eg: hand) • Laying on limb for long period of time –patient “found down” • Long surgery • Brown urine
What to Watch for if you suspect Rhabdo: • Clinical: Mm pain, weakness, dark urine • Hypovolemia, shock • Electrolyte abnormalities : ↑K+, ↓ Ca++ (sequestered in injured tissues), acidemia upon reperfusion
Clinical and laboratory features of rhabdomyolysis • History and physical examination • Urinalysis • Serum potassium concentration • Creatine kinase • Acid –Base balance • Uric acid • BUN/Cr • Ca/Ph methabolism • DIC
sample UA (+) for blood uric acid crystals Diagnosis • Serum CKMM • Correlates w/severity of rhabdo • Normally 145-260 U/L • Levels peak w/in 24h • >3000 high correlation with renal failure • #’s in 100,000’s not uncommon • high t(1/2): 1.5 days • Serum myoglobin • t(1/2) 2-3 h • Excreted in bile • Ca++ • UA-myoglobinuria • dipstick will be (+) for hemoglobin, RBC’s and myoglobin • Microscopy: no RBC’s, brown casts, uric acid crystals • Other measures: carbonic anhydrase III, aldolase
Approach to the patient with red or brown urine Electrolyte abnormalities
Muscle enzymes • The hallmark of rhabdomyolysis is an elevation in serum muscle enzymes. Serum CK levels may be massively elevated to above 100,000 IU/L. • Elevations in serum aminotransferases are common and can cause confusion if attributed to liver disease.
MANAGEMENT • Plasma volume expansion with intravenous isotonic saline should be given as soon as possible, even while trying to establish the cause of the rhabdomyolysis. • Treatment of the underlying cause of the rhabdomyolysis.
Monitoring with serial measurements of serum potassium, calcium, phosphate, and creatinine ,CPK is recommended.
MANAGEMENT • The metabolic consequences of and renal functional impairment due to rhabdomyolysis should be anticipated, particularly potentially life-threatening hyperkalemia. • Hypocalcemia? Should be treated?
Early Treatment • FLUIDS • Begin early, even on the field • Damaged muscles attract a lot of fluid • Up to 10L/day • Ideally NS with bicarb • prevents tubular precipitation • reduces risk of hyperkalemia from damaged mm • corrects academia • mannitol • renal vasodilator • free radical scavenger
Late Treatment • Dialysis – • intermitted preferred to continuous • Reduce use of anticoagulants in trauma patients