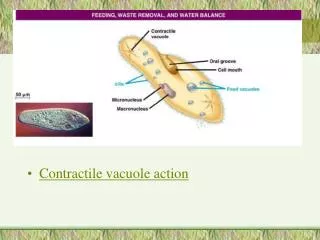
Reducing derangements Progressing contractile dysfunction
Reducing derangements Progressing contractile dysfunction. Mechanical Diagnosis and Therapy The lower extremit y. Mark Miller Beata Smela Jerry Pica Richard Rosedale. Guest: Karim Khan. MDT –The Peripheral Joints. HISTORY.


Reducing derangements Progressing contractile dysfunction
E N D
Presentation Transcript
Reducing derangementsProgressing contractile dysfunction Mechanical Diagnosis and Therapy The lower extremity Mark Miller Beata Smela Jerry Pica Richard Rosedale Guest: Karim Khan
MDT –The Peripheral Joints HISTORY
McKenzie, R.A., The Lumbar Spine: Mechanical Diagnosis and Therapy, 1981 “With this book I present a new concept of diagnosis for the whole musculo-skeletal system.”
McKenzie, R.A., The Lumbar Spine: Mechanical Diagnosis and Therapy, 1981 “The procedures I developed for the lumbar spine to arrive at appropriate conclusions regarding diagnosis and treatment, may also be applied successfully to the thoracic and cervical spine, and indeed to all peripheral joints and their surrounding soft tissues.”
The Peripheral Joint Problem • too common • too persistent • too frustrating • current treatments • assessment reliability • assessment validity
The Peripheral Joint Problem(cont’d) • MRI - 32%-44% rotator cuff tears • MRI – 60% medial meniscal tears • MRI – 61.4% Knee OA abnormalities • MRI – 58% Labral lesions
McKenzie’s Solution Mechanical Diagnosis and Therapy Historical analysis + Mechanical assessment
MDT and The Utah Paradigm Changing Concepts in Skeletal Physiology: Wolff’s Law, the Mechanostat, and the ‘‘Utah Paradigm’’ HAROLD M. FROST*AMERICAN JOURNAL OF HUMAN BIOLOGY 10:599–605 (1998)
“Biological Baseline” set at birth Mechanical forces generate signals in skeletal tissues Control the biologic mechanisms and determine the architecture and strength of those tissues
These occur in ways that let tissues endure their voluntary mechanical usage for life without hurting or breaking To work properly, these mechanisms need non-mechanical factors (hormones, vitamins, calcium, etc.), However…
Mechanical factors can guide those mechanisms in time and anatomical space This arrangement determines musculoskeletal health…the mechanical forces can help or hinder
If these mechanical factors are excessive, inadequate or inappropriate Tissue weakness Tissue breakdown Joint derangement
MDT Implications • Use of optimum amount of mechanical load • In the appropriate starting position • In the correct direction • For enough time Restoration of Musculoskeletal Health
Extremity Examples in the Literature • A. Aina, S. May Manual Therapy 10 (2005) 159–163 Shoulder Derangement Reduction
Extremity Examples in the Literature • S.J. Horton, A. Franz Manual Therapy(2007) 12 (2) SIJ Derangement Reduction
Load DOES matter Become a “load master” The Load Colin Davies, PT, Dip. MDT Volume 2, No. 1 March 2007 International Journal of Mechanical Diagnosis and Therapy
Reducing derangementsProgressing contractile dysfunction Mechanical Diagnosis and Therapy The lower extremity
Tendinopathy Degeneration Mechanotransduction
Stages of tissue healing Inflammatory: 1-5 days prepares area for repair Repair & Healing: three weeks rebuilds the structure Remodeling: up to 6 weeks-12 months provides final form of the scar
REMODELING Wolff’s lawBland’92 Bone will remodel with loading – Nordin & Frankel ’89 Muscle will hypertrophy – Pitman, Peterson ’89 • Anatomical structures and tissues will tend to reflect functional stresses demanded on them
REMODELING Compressed tendon was replaced by hyaline cartilage Tension to the tendon reversed it back to the tendon structure (Merrilees & Flint 1980) In animal model:
Non-specific diagnosis ? “..Within physiotherapy, management is often determined by a patient’s impairment and the stage of the disorder rather than a specific tissue diagnosis…”. Jette, Delitto’97, van Baar’98, Dekker’93
State of tissue Pain mechanism Abnormal stress / mechanical Normal Predominantly chemical Inflamed Chemical/mechanical interface Healing Abnormal / Contracted Mechanical Mechanical Abnormal / Derangement Persistent hypersensitivity Peripheral / central sensitization
Mechanical diagnosis Postural Dysfunction– articular, contractile Derangement Neural tissue malfunction Other
Contractile dysfunction DEFINITION: Pain resulting from mechanical deformation of structurally impaired contractile tissues as a result of trauma, inflammation or degeneration.
Patternbased diagnosis and management INTERMITTENT PAIN duration> than 6 weeks PRODUCED consistently, locally with resistive load NO WORSE with repetition MECHANICS No immediate change with repeated resistive load on: • Range • Strength • Function
Management of mechanical pain Medications SHOULD Never BE THE FIRST TREATMENT CHOICE
Clear model of acceptable pain behavior in response to loading Localization Spreading Pain lasting no longer than 10 minutes following treatment
Loading contractile dysfunction Active Movements Isometrics (precautions) Resisted (Concentric / Eccentric) TARGET ZONE (outer range/inner range) Amplitude Speed REMODEL
Decline board (25 degrees) Balance board Back pack Weighted vest / belt Exercise machines, t-band Different starting positions Assisted / deloading Taping, straps, braces Shoe lifts Sound muscles - concentric, affected muscles - eccentric (Opposite leg up, affected down) Other creative choices Loading/ deloading ideas
Decline board Young 2005, Kongsgaard 2006, Visnes 2007
How to do it ?Loading selectionYOUNG 2006 (knee) • Decline board group: 2 x daily, x 12 weeks, 60 degrees flexion, down painful leg, up on sound leg, moderate pain, back pack at 5 kg increments when pain eased • Box squat group: as above except painful leg up/down, minimal pain, progress speed slow to fast
Loading selectionSilbernagel 2007 (Achilles) • once a day for 6 months, reps? • on the floor to the edge of the step • two-legged concentric/ eccentric toe raises • eccentric fast rebounding toe- raises • increase repetitions • increase load ( back pack, machine) • plyometric training
Loading selectionAlfredson (Achilles) • Eccentric loading with straight and bent knee • 15 x3set, 2 times per day for 3 months • More pain the first two weeks, the exercise must be painful
Loading selectionMcKenzie May 2003 (any contractile dysfunction at middle portion) • 5-12 repetitions, 3-4 x a day at target zone progress to 10 repetitions every 2 hours produce concordant pain - no worse ( 10 min resolution following exercise) • Force alternatives (eccentric > concentric, above/ below target zone, angle of the joint, angle of the board, external load, speed, simulate desired function
Return to function - timeframe 2 to 6 months
Barriers to recovery Lack of early mobilization Inadequate stress (no gradation of exercises and daily activities) Ongoing inflammation (primature activation) Poor timing or choice of passive modalities or orthoses Using prolonged versus intermittent stress (Hardy ’89) Failure to restore the desired function (especially in athletes) Training errors (technique, plyometrics, muscle imbalances)
Barriers to recovery Local steroid Poor blood supply or ischemia, high tissue pressure with immobilization Poor nutrition Keloid formation or scar shortening Nodules of abnormal tissue with nerve infiltration (Cousins ’94, Hardy) Suspended healing Age Fear –avoidance, poor coping, anxiety, external locus, sick role etc.
Fibrocartilage enthesis Tendon undergoes compressive forces Poor response to tensile forces Loading selection? Bone/tendon junction - Enthesis
Outcome measures • VISA (Victorian Institute of Sport Assessment) • VISA –A (Achilles) • Lower Limb Functional Scale • Lysholm Knee Scale • VAS (Visual Analog Scale) • Functional tests: CMJ (counter movement jump) drop, vertical, max power concentric/ eccentric toe-raise, endurance test with weighted belt Other: • 3 functions that are limited (rate in % of subjective recovery)
“ Full symptomatic recovery does not ensure full recovery of muscle –tendon function in patients with Achilles tendinopathy ”.Silbernagel KG, THomee R, Ericksson BI, KArlsson JBritish Journal of Sports Medicine 2007, 41
Group work Mechanical differential diagnosis