Participant Questions
This overview presents vital findings from two recent studies related to acute venous thromboembolism (VTE) prevention, focusing on the impact of concurrent statin therapy. The JUPITER study demonstrated that rosuvastatin significantly reduced the risk of first VTE in a diverse population over a median follow-up of 1.9 years. Additionally, we detail the relationship of biomarkers and clinical scoring systems in assessing acute pulmonary embolism (PE) risks, emphasizing their roles in guiding treatment decisions and improving outcomes in high-risk patients.

Participant Questions
E N D
Presentation Transcript
Participant Questions 1. Concurrent anti-platelet therapy with VKA or LMWH?
VTE Wild Card:Two Studies You May Have Missed Matthew Rondina, MD University of Utah
JUPITER Study Design • N=17,802 healthy men and women • LDL < 130 mg/dL and hs-CRP ≥ 2.0 mg/L • Randomized to rosuvastatin 20mg daily or placebo • Median FU: 1.9y (max 5 yrs) • Occurrence to first VTE protocol-specified secondary endpoint • Intention-to-treat analysis Glynn RJ et al. N Eng J Med 2009;360:1851-61
Rosuvastatin 20mg Daily Reduced Risk of First VTE Glynn RJ et al. N Eng J Med 2009;360:1851-61
Effect Consistent Across Subgroups • Similar to reduction in arterial events • No association with LDL, HDL, TG, hs-CRP • Similar reductions for provoked and unprovoked VTE • No significant difference on early vs late events (>24 mos) • Effect consistent across subgroups • Gender • Age • BMI, waist circumference • Metabolic syndrome Glynn RJ et al. N Eng J Med 2009;360:1851-61
Expands role of statins for 1º VTE prevention Unknown if any benefit for 2º prevention May be statin-specific + Rosuva, ? + Simva No effect with pravastatin Suggested, but unproven, uses: VTE prophylaxis in cancer 2º prevention where AC is contraindicated Should Statins Be in the Water? N Eng J Med 2009;360:1851-61 JTH 2004;2:700-1 JTH 2004;2:695-6 JTH 2006;4:1925-7
In Search of the Holy Grail in Acute Sub-Massive PE:Can We Further Refine Our Ability to Risk Stratify?
Pulmonary Embolism May Lead to Sudden Cardiovascular Collapse Acute PE Pulmonary HTN RV Function RV Volume LV under-filling: hypotension RV Pressure Micro-infarction Shear Stress
Hypotension Normal BP, + RVD/RVE Normal BP Nl biomarkers No RVD/RVE
Clinical Risk Stratification for Acute PE: Geneva Risk ScorePE Severity Index Cancer Age Heart failure Male Sex Previous DVT Cancer Systolic Pressure <100 Heart Failure pa02 < 8 kPa Chronic lung disease DVT on US Pulse rate >100/min Systolic Pressure <100 Resp Rate >30/min Temp < 36 degrees C Altered mentation Sa02 <90% Low Risk30d mortality GRS 84% 5.6% PESI 36% 0.9% Arch Intern Med 2006;166:169-175 JIM 2007; 261:597 CHEST 2007; 132:24 Thromb Haem 2008; 99:502
Pulmonary Embolism: Biomarker-Based Risk Stratification Natriuretic PeptidesTroponin I/T Mortality ?? 5-fold PPV 12-23% 12-44% NPV 99-100% 97-100% Assay Variation Standardized Nl Range Variation Standardized Data + +++ Circ 2003;108:2191-2194 Circ 2007;116:427-433 Chest 2008;133:1531-2 Chest 2008;133:334-6 Chest 2009;136::974-982
Pulmonary Embolism:RVE Increases Mortality Risk • RV Enlargement by Echo: • Defined as a RV diameter > 90% of the LV diameter in the long axis view • Associated with 6.6% in hospital mortality (vs. 1.9%; 2.6x risk) • Associated with 47% 30-day survival (versus 71% if normal RV diameter) • When combined with elevated TnI, 30-day survival is only 25% • Noninvasive and no contrast but may not be available 24/7 in all centers Chest 2008; 133:358-362 Chest 2008;133:334-336 Am J Card 2005;96:303-305
TELESIO: Identify High-Risk APE Pts?201 Prospective, consecutive APE Pts and SBP≥90 • Clinical score: Geneva Risk Score (≥3 points) • TTE: RVE, PAP>34 mmHg, and/or RV hypokinesis* • Trop-I • Beckmann: nl<0.07 ng/mL or 20xULN • Dade: nl<0.15 ng/mLor 20xULN • BNP • Roche/Elecsys: nl<100 pg/mLor 10xULN • D-Dimer • Roche/Star: nl<250 ug/mL or 6xULN *RVD required either one or all three (restrictive criteria) J Thromb Haemost 2009;7:938-944.
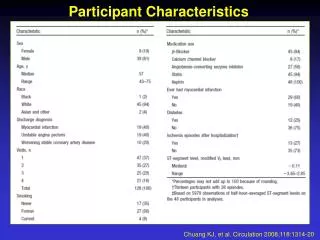
Abnormal Prognostic Markers Were Common…. J Thromb Haemost 2009;7:938-944.
But Did Not Predict In-hospital PE-related Mortality or Clinical Deterioration IP PE-Death IP All Death 3-Mo All Death [N=1, 0.5%] [2%] [9%] RVD --- --- --- RVD3 --- --- --- BNP --- --- --- BNP10 --- --- --- D-Dimer 6 --- --- + GRS* --- + + Trop-I* --- + + Trop-I 20 --- --- --- Hypoxemia --- + + J Thromb Haemost 2009;7:938-944.
3-Month Mortality Best Predicted by Clinical Score or Troponin-1 J Thromb Haemost 2009;7:938-944.
Are Prognostic Markers Useful for Identifying Higher-Risk APE for Thrombolytics? • Did not predict in-hospital PE-related AE • Did not predict 3-month PE-related mortality or VTE recurrence • May not be useful as guide to more aggressive therapy in APE with SBP ≥ 90 • Did predict 3-month all cause mortality • May reflect underlying comorbidities • Patients with normal markers had benign hospital course • Authors did not assess other outcomes • Exercise intolerance or dyspnea at rest • Persistent RV dysfunction or pulmonary HTN Bova et al, J Thromb Haemost 2009;7:938-944 Kline JA. J Thromb Haemost 2009; 7: 1601–2 Kline JA et al. Crit Care Med 2006; 34: 2773–80.