Download
1 / 62
630 likes | 872 Vues
Inflammatory and Valvular Heart Diseases. Rheumatic Fever and Heart Disease. Rheumatic Fever - inflammatory disease of heart potentially involving all layers Systemic Abnormal immune response to group A beta hemolytic strep (“strep throat”) Transmission to heart via lymphatic channels

E N D
Rheumatic Fever and Heart Disease • Rheumatic Fever - inflammatory disease of heart potentially involving all layers • Systemic • Abnormal immune response to group A beta hemolytic strep (“strep throat”) • Transmission to heart via lymphatic channels Most common cause of valvular heart disease
Rheumatic Fever and Heart Disease • Rheumatic Heart Disease – chronic condition characterized by scarring and deformity of heart valves resulting from rheumatic fever • Any or all layers of heart maybe affected
Rheumatic Fever and Heart Disease • Rheumatic endocarditis (most serious) • Erosion and swelling of valves (thickening) • Vegetations • Stenosis/Regurgitation • Rheumatic Myocarditis • Nodules and fibrin deposits loss of contractile powerCHF • Rheumatic Pericarditis • Fibrinous Exudate and pericardial effusion
Rheumatic Fever and Heart Disease • Nursing Assessment • Previous history of rheumatic fever • Socioeconomic class • Fever • Cardiovascular (tachycardia; pericardial friction rub; distant heart sounds; murmurs) • Neurological: chorea • Skin: subcutaneous nodules and erythema marginatum • Musculoskeletal: Polyarthritis
Rheumatic Fever and Heart Disease • Primary Prevention • Detection and treatment of strep throat • Secondary Prevention • Prophylactic antibiotics to prevent recurrent ARF
Rheumatic Fever and Heart Disease Acute Intervention • Antibiotics • Rest • Control Fever • Anti-Inflammatories
Infective Endocarditis • Infection of the inner layer (endocardium) of the heart that usually affects the cardiac valves • Was almost always fatal until development of penicillin • 5,000-8,000 cases diagnosed in U.S. each year
Classification • Subacute form • Longer clinical course • Insidious onset • Streptococcus bovis or viridians • Staphylococcus epidermidis • HACEK group
Classification • Acute form • Shorter clinical course • Rapid onset • Causative organism more virulent • Streptococcus pneumoniae • Staphylococcus aureus • Streptococcus groups A, B, C • Fungi
Etiology and Pathophysiology • Vegetations • Fibrin, leukocytes, and microbes • Adhere to the valve or endocardium • Embolization of portions of vegetations into circulation
Etiology and Pathophysiology • Left-sided more common with bacterial infections and underlying heart disease • Right-sided lesions usually caused by IV drug abuse
Etiology and Pathophysiology • Risk Factors: • Cardiac Conditions (blood flow turbulence allows pathogen to infect previously damaged valves or other surfaces) • Rheumatic heart disease • Prosthetic valves • Aging • IV drug abuse • Invasive Medical and Dental Procedures • UTI, skin/wound infections
Clinical Manifestations • Nonspecific • Fever occurs in 90% of patients • Chills • Weakness • Malaise, Fatigue • Anorexia
Clinical Manifestations • Vascular manifestations • Splinter hemorrhages in nail beds • Petechiae • Osler’s nodes on fingers or toes • Janeway’s lesions on palms or soles
Clinical Manifestations • Murmur in 80% of cases • CHF • in up to 80% with aortic valve endocarditis • 50% with mitral valve endocarditis • Manifestations secondary to embolism
HISTORY • Recent dental, urologic, surgical, or gynecologic procedures • Heart disease • Recent cardiac catheterization • Skin, respiratory, or urinary tract infections
Diagnostic Studies • Labs • Blood cultures • Echocardiography (detects valvular vegetations, abscesses) • Chest x-ray
Collaborative Care • Prophylactic treatment for patients having: • Removal of drainage of infected tissue • Indwelling pacemakers • Renal dialysis • Ventriculoatrial shunts
Collaborative Care • Antibiotic administration • Monitor antibiotic serum levels • Antipyretics • Subsequent blood cultures • REST • Valve repair/replacement
Nursing Assessment • Subjective • History of valvular, congenital, or syphilitic cardiac diseases • Previous endocarditis • Staph or strep infection • Immunosuppressive therapy
Nursing Assessment • Recent surgical procedures or invasive procedures • IV drug abuse • Weight changes • Chills • Diaphoresis
Nursing Assessment • Bloody urine • Exercise intolerance • Generalized weakness • Fatigue • Cough • Dyspnea on exertion • Night sweats • Chest, back, abdominal pain
Nursing Assessment • Objective • Olser’s nodes • Splinter hemorrhages • Janeway’s lesions • Petechiae • Clubbing
Nursing Assessment • Tachypnea • Crackles • Arrhythmias • Leukocytosis • Increased ESR and cardiac enzymes • Positive cultures • ECG showing chamber enlargement
Nursing Diagnoses • Decreased cardiac output • Activity intolerance • Ineffective health maintenance
Acute Pericarditis • Caused by inflammation of pericardial sac • Etiologies: Infectious vs Non-Infectious • S&S: dyspnea, CP, pericardial friction rub • Complications • Pericardial effusion • Cardiac tamponade • Treatment • Antibiotics • NSAIDS • Corticosteroids • Positioning head at 45 degree angle • Pericardiocentesis
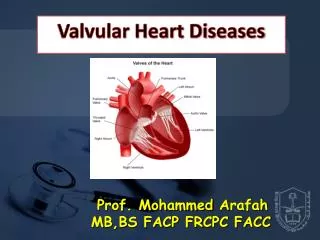
Valvular Heart Disease • Heart contains two atrioventricular valves and two semilunar valves
Valvular Heart Disease • Types of valvular heart disease depends on: • Valve or valves affected • Two types of functional alterations • Stenosis • Regurgitation
Valvular Heart Disease • Stenosis • Valve orifice is restricted • Impending forward blood flow • Creates a pressure gradient across open valve • Degree of stenosis reflected in pressure gradient differences • Regurgitation • Incomplete closure of valve leaflets • Results in backward flow of blood
Mitral Valve Stenosis • Due to rheumatic heart disease • Causes scarring of valve leaflets and chordae tendineae • Contractures develop with adhesions between commissures of the leaflets • Stenotic mitral valve assumes funnel shape due to thickening and shortening of valve structures
Mitral Valve Stenosis • Pathophysiology: • Incomplete emptying of LA Increased LA pressure LA dilatation and hypertrophy • Increased LA pressureElevated pulmonary pressurepulmonary congestion • Incomplete emptying of LAinsufficient volumes to ventricles decreased C.O. • Afib is common risk of embolism
Clinical Manifestations • Dyspnea • Occasionally accompanied by hemoptysis • Primary symptom because of reduced lung compliance • Palpitations from atrial fibrillation • Fatigue • Opening snap • Low-pitched rumbling diastolic murmur • Chest pain • Seizures (from emboli) • Stroke • Emboli can arise from stagnant blood in left atrium
Mitral Valve Regurgitation • Mitral Valve fails to close properly • LV ejects blood into aorta and back into LA
Mitral Valve Regurgitation • Majority of cases attributed to: • MI (MI with left ventricular failure places patient at risk for rupture of chordae tendineae) • Chronic rheumatic heart disease • Isolated rupture of chordae tendineae • Mitral valve prolapse • Ischemic papillary muscle dysfunction • Infectious endocarditis
Mitral Valve Regurgitation • Acute Onset (e.g. papillary dysfunction due to M.I.) • Backward flow increased LA pressure Increased Pulmonary Pressure Pulmonary Edema • Chronic Onset • Backward flow LA dilates and hypertrophies Increased pulmonary pressures pulmonary congestion right sided failure
Mitral Valve RegurgitationClinical Manifestations • Asymptomatic for years until development of some degree of left ventricular failure • Initial symptoms include: • Weakness • Fatigue • Dyspnea that gradually progress to orthopnea, paroxysmal nocturnal dyspnea, and peripheral edema
Aortic Valve Stenosis • Usually discovered in childhood, adolescence, or young adulthood • Those seen later in life usually have aortic stenosis from rheumatic fever or senile fibrocalcific degeneration of a normal valve
Aortic Valve Stenosis • Results in obstruction of flow from LV to aorta during systole • Effect is left ventricular hypertrophy and increased myocardial oxygen consumption because of increased myocardial mass • Leads to reduced CO and pulmonary hypertension
Aortic Valve StenosisClinical Manifestations • Symptoms of angina pectoris • Syncope • Heart failure • Occurs when valve orifice is 1/3 normal size
Aortic Valve Stenosis • Poor prognosis when experiencing symptoms and valve obstruction is not relieved • Why would Nitroglycerine be contraindicated with aortic valve stenosis?
Aortic Valve Regurgitation • May result from disease of aortic valve leaflets, aortic root, or both • Caused by: • Bacterial endocarditis • Trauma • Aortic dissection • Constitutes life-threatening emergency • Chronic aortic regurgitation results from: • Rheumatic heart disease • Congenital bicuspid aortic valve • Syphilis • Chronic rheumatic heart conditions
Aortic Valve Regurgitation • Physiologic consequence: • Retrograde blood flow from ascending aorta to left ventricle • Elevated LV pressures • LV dilatation and hypertrophy • Results in volume overload
Tricuspid Valve Disease • Tricuspid valve stenosis • Seen in IV drug users • Right atrial output is obstructed • Results in right atrial enlargement and elevated systemic venous pressure
Tricuspid Valve DiseaseClinical Manifestations • Peripheral edema • Ascites • Hepatomegaly • Murmur
Collaborative Care • Drug therapy • Digitalis • Diuretics • Antiarrhythmics • b-blockers • Anticoagulants • Low-sodium diet