Download
1 / 40
400 likes | 556 Vues
Spinal Tumors: A Second Chance at Life. Angela Sarro, RN(EC), MN, CNN(c) Nurse Practitioner-Adult Spine Program Toronto Western Hospital University Health Network. Objectives. To understand decision making with spinal tumor resections

E N D
Spinal Tumors: A Second Chance at Life Angela Sarro, RN(EC), MN, CNN(c) Nurse Practitioner-Adult Spine Program Toronto Western Hospital University Health Network
Objectives • To understand decision making with spinal tumor resections • To appreciate surgical approaches and potential complications • Understand potential impact on quality of life • Integration of case study throughout
Diagnosis of spinal tumor can be overwhelming and anxiety provoking • Long term outcomes are variable depending on presenting symptoms, tumor type and treatment options • Treatment options depend on type and location of tumor: • Observation • Surgical resection • Chemotherapy • Radiation • Medications
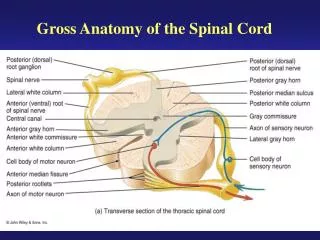
Clinical Presentation • Back pain • Persistent and progressive • Worse at night • History of cancer** • Neurological symptoms • Loss of sensation or muscle weakness in arms or legs • Decreased sensitivity to pain, heat or cold • Difficulty walking, possible falls • Loss of bowel or bladder function • Paralysis
Case Study • Mr. S. • 58 year old male • Complaints of neck pain and mild dysphagia for 1 year • Worked up by family MD • Presents to spine clinic with dysphagia
PMHx • HTN • Glaucoma left eye • A-fib arrest 2003 • Cardiac stenting • No issues since • No known allergies
Radiological findings • Large retropharyngeal mass • Tumor largely anterior but did involve posterior elements • Involved C2 vertebral body and peg extending down to body C3 • Tumor encased vertebral artery bilaterally at C3 • Felt to be a chordoma
C3 vertebral body involvement C2-C3 with bilateral vertebral artery involvement
Primary Benign Tumors Osteoid osteoma Osteoblastoma Osteochondroma Aneurysmal bone cyst (ABC) Giant cell tumor Primary Malignant Tumors Chondrosarcoma Osteosarcoma Ewings sarcoma Chordoma Types of Tumors • Common Metastatic Spinal Tumors • Breast Prostate Lung Renal Gastric
En Bloc Resection • En bloc resection with adequate margins is associated with the highest probability of long-term tumor control or cure in cases of primary tumor • Goal: negative margins • No intra-lesional dissection • Chance for longer survival knowing that function will not be “normal”
Feasibility of en bloc resection is determined by careful surgical and oncologic staging • Key step in this process is obtaining a tissue diagnosis • Experienced, multidisciplinary teams should perform these surgeries
Surgical Approaches • Need to determine extent of involvement of tumor with spine, adjacent soft tissue or organs • Location of tumor will determine surgical approach/approaches • May require multidisciplinary approaches • Often done in two stages due to complexity • Stage 1 – Posterior • Stage 2 – Anterolateral/Posterior
Pre-op Preparation • Local and systemic staging to rule out nodal or distant disease especially in cases of metastatic disease • Sometimes treated with chemotherapy and radiation pre-op depending on tumor sensitivity and/or previous treatments • Restaged following treatment prior to en bloc excision to re-evaluate tumor size and minimize extent of surgery
Patient Selection • No epidural involvement • Reasonable medical condition • Patient awareness of magnitude of surgery and length of recovery
Patient Discussion • Magnitude of surgery • Complication rate up to 30% • UTI • Infection • Pneumonia • DVT/PE • Prolonged hospital stay • Likelihood for need of rehab following acute care
Many patients have NO pain pre-op • Need to be aware that there will be pain post-op and likely life-long • Possible deficits if nerve roots are part of dissection • Trade off for longer lifespan
Pre-op Discussion with Mr. S. • Primary malignant tumor – chordoma • Best approach would be en bloc resection • Complex procedure • Two stage process to enable en bloc resection • Functional loss • Long-term pain • Complications
Likelihood of adverse event 30% or higher • UTI • Pneumonia • Infection, CSF leak • Hardware failure • Brain stem or spinal cord stroke • Peri-operative tracheostomy and gastrostomy tube • Involvement of: • ENT • Neurosurgery • Spine • Length of hospital stay and need for rehab
En BlocTechnique • Evolved over review • Current preference: two stage procedure • 1st: posterior instrumentation, release of tumor • 2nd: combined anterior and posterior approach
Surgical Resection • Preserve superficial ± deep paraspinals to provide coverage post resection • Depending on tumor location: • Release discs, facets, ribs • Ipsilateral hemi- laminectomies, ligation nerve roots • Ligation of blood vessels • Removal of other organs
Length of surgical procedure is very long • Stage 1: 5-6 + hrs • Stage 2: Actual tumor resection and removal can be 10 + hours
Surgical Procedure Mr. S. • Stage 1 • Tracheostomy • Posterior approach • Vertebral artery bypass by neurosurgery • Left side bypass graft (easiest to access) utilizing right saphenous vein • Occlusion right vertebral artery • SSEP monitoring • Total OR: 24 hours
Stage 2 • Postponed for 4 weeks secondary to: • extensive facial swelling and coagulopathy (controlled) • CNS altered sensorium which resolved • Transmandibular split with en bloc resection of tumor • Small dural tear repaired at time of surgery • Vascularized fibular graft
Posterior instrumentation Vascularized fibular graft Tracheosotomy
Post-op Considerations in General • Respiratory • Possible intubation post-op • Tracheostomy • Atelectasis • Pneumonia • Vascular • DVT/PE • Gastrointestinal • Nutritional support • Bowel function
Skin Integrity • Early mobilization • Astute skin assessment • Pressure relieving surfaces • Wound healing
Pain Management • Involvement of Acute Pain Service • Epidural catheter • IV Patient controlled analgesia • Transition to oral medications • Mobility • Followed by PT/OT • Likelihood of inpatient rehabilitation quite high
Complications Mr. S. • Decreased LOC post-op Stage 1 • r/o cerebral event • Facial swelling • Secondary to long prone position Stage 1 • GI bleed • Arrhythmia • Pneumonia • UTI • C-difficile infection
Dysphagia • G-tube insertion • Ongoing aspiration with attempts at oral feeds • Palatal fistula • Weak right vocal cords • Will require permanent g-feeds
Mr. S. sent to rehab in halo vest for added support to surgical reconstruction • Stage 3 • Done 7 months later to place posterior bone graft to augment anterior fibular graft for further anatomical support • 12 cm length of rib utilized • ENT also repaired palatal fistula at the same time
CT Post-op Stage 3 Posterior rib graft
Overall Course Treatment • Initial hospitalization was 5 1/2 months • Followed by rehab for 5 weeks • Second hospitalization 4 weeks • Seen at regular intervals post-operatively • At 3 year mark (November 2011) remains cancer free • Continues to require g-feeds
Conclusion • Aggressive resections required • Curative resection obtainable • Lower complications seen with staged resection • Worse outcome attributable to morbidity of surgery or natural progression of disease • Probably not worth it if local disease cannot be fully controlled • Best outcome if respond to pre-op chemo and radiation • In the end, quality of life is often sacrificed for quantity