Download
1 / 15
150 likes | 291 Vues
PHARMACOKINETIC ANALYSIS OF TUBERCULOS DRUGS. Aylin Babalık, İsmail Hakkı Ulus, Nadi Bakırcı, Tülin Kuyucu, Hüseyin Arpağ, Lale Dağyıldızı Turkish Thoracic Society 15th annually Congress 11-15 April 2012. Conflict of interest. Turkish Thoracic Society Project support

E N D
PHARMACOKINETIC ANALYSIS OF TUBERCULOS DRUGS Aylin Babalık, İsmail Hakkı Ulus, Nadi Bakırcı, Tülin Kuyucu, Hüseyin Arpağ, Lale Dağyıldızı Turkish Thoracic Society 15th annually Congress 11-15 April 2012
Conflict of interest Turkish Thoracic Society Project support The Turkish Academy of Science Project Support KaanMedikal Laboratory
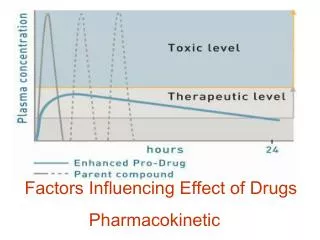
Aim • Monitoring plasma drug levels is useful and necessary to achieve maximal effect and avoidance of toxic side effects of drugs. • Knowledge of changing blood levels is necessary for drug level monitoring. • The aim of this study is to determine the changes in Tuberculosis drug levels over a period of time. • Peloquin CA. Therapeutic drug monitoring in the treatment of tuberculosis. • Drugs. 2002;62:2169-83
Pharmacokinetic parametres of the antituberculosis drugs • Peloquin CA. Therapeutic drug monitoring in the treatment of tuberculosis. • Drugs. 2002;62:2169-83.
Inclusion and Exclusion Criteria • Ekslusion • Disease caused by atypical Mycobacteria,, • Multidrug-resistant tuberculosis treated with second-line agents, • Under the tuberculosis treatment cases, • Patients who had co-morbidity disease, • Patients who had serum creatinin > 200µmol/l Inclusion • smear- or culture-positive Mycobacterium tuberculosis hominis pulmonary tuberculosis or patients who had clinical and radiologic tuberculosis definition. 21 Tuberculosis patients who had no co-morbidity disease (11 male, 10 female; average age 38,1 ±17.0) were included in this study between March-May 2011.
Material ad Methods • Blood was drawn after administering INH ( 5mg/kg), RIF (10mg/kg), EMB (25 mg/kg) and PZA (25 mg/kg) on the 1st hour, 2nd hour, 4th hour, 6th hour, and 24th hour during fasting. Plasma drug level was measured with liquid chromatography.Drug levels are expressed with means±SD. • Blood was drawn after administering INH ( 5mg/kg), RIF (10mg/kg), EMB (25 mg/kg) and PZA (25 mg/kg) on the 1st hour, 2nd hour, 4th hour, 6th hour, and 24th hour. • Plasma drug level was measured with liquid chromatography. • Blood drug level mean± standart error, median, minimum, maksimum
Table 1: Patients characteristics before the start of treatment
Pharmacokinetics of anti-tuberculosis drugs After first administration
Pharmacokinetics parameters of isoniazid, rifampin, pyrazinamide and ethambutol in tuberculosis patients
Anti-tuberculosis drugs blood levels after beging treatment on 1st, 14th,30rd at 2nd hour
CONCLUSIONS • These results shows big individual differantial on drug levels and calculated Pharmacokinetics parameters. • Although there was not statistically diffrential, INH blood levels on female, PZA blood levels on male, at some time interval were lower. After RMP administration, time of Cmax was more delay. Unfortunately, at this study, number of study population was not enough for compare gender. More confident results will be achieved if case number increase.
CONCLUSIONS 3. These results show INH, RIF, EMB and PZA increased maximal level on the 2nd hour after oral administration of the drugs. The 2nd hour is an appropriate time for monitoring four of the therapeutic drug levels. 4. Cmax values was under therapeutic levels At Most of patients .(POSTER:Blood levels of tuberculosis drugs and affecting factors of drug levels) This result become suspicious for affectivity of anti-tuberculosis drugs 5. . Treatment outcomes is evaluating. Treatment outcomes evaluating With Under these results will give important results