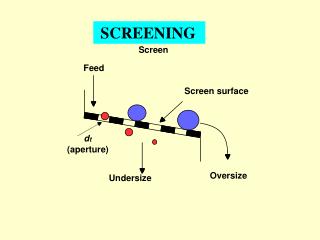
FUNCTIONAL MOVEMENT SCREENING
FUNCTIONAL MOVEMENT SCREENING. Gross limitation of fundamental movement patterns, even if pain free, can cause compensation and substitution leading to poor efficiency , secondary problems and increased injury risk. Basic principles of functional movement systems.

FUNCTIONAL MOVEMENT SCREENING
E N D
Presentation Transcript
Gross limitation of fundamental movement patterns, even if pain free, can cause compensation and substitution leading to poor efficiency , secondary problems and increased injury risk.
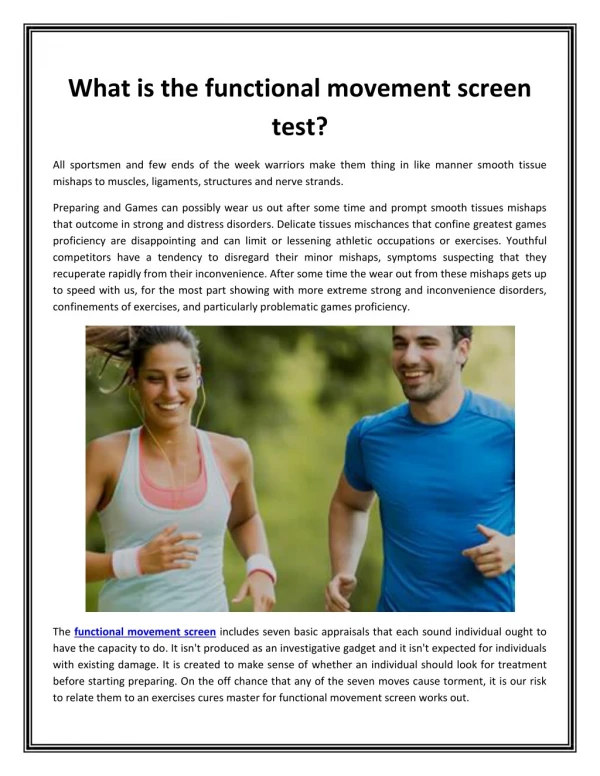
Basic principles of functional movement systems • Basic bodyweight movement patterns should not provoke pain. If pain is present in movement, activity and exercise should be modified, interrupted or stopped as additional information is gathered. If not compensation and altered movement patterns can result, and these are likely to aggravate the problem and cause secondary movement problems if left unaddressed • Pain regardless of its origin affects motor control.
Basic principles of functional movement systems • Fundamental movement patterns involving the body’s left and right sides should be mostly symmetrical. • Fundamental movement capability should precede performance based capability. don’t load up dysfunction
Basic principles of functional movement systems • Fundamental movement capability should mostly precede complex activity or complex skill training. These movements form a neuromuscular foundation for advanced lifters/athletes and reduce the need for compensation and substitution often observed when fundamental movement is limited.
Top risk factor for injury? • Previous injury • A lot of physical therapist treat their client until the pain is gone but may not correct the movement pattern that caused the pain. • Valgus collapse – could be pain free but dysfunction still exist
Movement screening test • Deep squat • Hurdle step • Inline lunge • Shoulder mobility • Active straight leg raise • Trunk stability pushup • Rotary stability
http://graycookmovement.com/?p=68 • Programming based on your movement profile • All of your clients can do this
Deep squat • Demonstrates fully coordinated extremity mobility and core stability, with the hips and shoulders functioning in symmetrical positions • Used to test bilateral, symmetrical, functional mobility and stability of the hips, knees and ankles • The dowel held overhead calls on bilateral symmetrical mobility and stability of the shoulders, scapular region and the thoracic spine.
Implications • Limited mobility in the upper torso can be attributed to poor glenohumeral or thoracic spine mobility, or both • Limited mobility in the lower extremities, including poor closed kinetic chain dorsiflexion of the ankles or poor flexion of the knees and hips can cause poor test performance • Poor stabilization and control
HURDLE STEP • Challenges the body’s step and stride mechanics, while testing stability and control in a single leg stance. • Excessive upper body movement in basic stepping is viewed as compensation; it is not seen when proper mobility, stability, posture and balance are available.
Implications • Problems may be due to poor stability of the stance leg or poor mobility of the step leg.
INLINE LUNGE • Requires appropriate starting stability and continued dynamic control of the pelvis and core within an asymmetrical hip position. • Challenges hip, knee, ankle, and foot mobility and stability. • http://www.youtube.com/watch?v=-XF7HqnFNwc&NR=1&feature=endscreen
Implications • ankle, knee and hip mobility may be inadequate for either the front or rear leg. • Dynamic stability may not be adequate to complete the pattern • There may also be limitations in the thoracic spine region, inhibiting the client from performing well.
Shoulder mobility • Demonstrates the natural complementary rhythm of the scapular –thoracic region, thoracic spine and rib cage during reciprocal upper extremity shoulder movements. • This pattern observes bilateral range of motion, combining extension, internal rotation and adduction in one extremity, and flexion, external rotation and abduction of the other.
Implications • Scapular stability depends on thoracic mobility. This should be the primary focus • Excessive development and shortening of the pectoralis minor, latissimusdorsi and rectus abdominus muscles (CAUSED BY SITTING ALL DAY) can cause the postural alterations of forward or rounded shoulders. This postural problem leaves unrestricted mobility of the glenohumeral joint and scapula at a disadvantage • Look for scapulothoracic dysfunction • CLEARING EXAM.
Active straight leg raise • Identifies the active mobility of the flexed hip and includes the initial and continuous core stability within the pattern as well as the available hip extension of the alternate hip. • Challenges the ability to dissociate the lower extremities while maintaining stability in the pelvis and core. Also challenges active hamstring and gastroc-soleus flexibility, while maintaining a stable pelvis and active extension of the opposite leg.
http://www.youtube.com/watch?v=EWNk7itK9oc&feature=related • Client lies supine with the arms by the sides, palms up and head flat on the floor. A board is placed under the knees. Soles of the feet should be perpendicular to the floor. Find the point between the anterior and superior iliac spine and the joint line of the knee and place the dowel in the position. Instruct the client to lift the test leg while maintaining the opposite leg in the starting position • If the malleolus passes the dowel the client gets a full score.
Implications • Pelvic control may not be sufficient for the execution of the pattern • The client may have inadequate mobility of the opposite hip, stemming from inflexibility associated with limited hip extension • The client may have poor functional hamstring flexibility in the moving limb • When the pattern is correct, the non moving limb demonstrates stability, an automatic task, while the moving limb demonstrates mobility, a conscious task.
Trunk stability pushup • Observation of reflex core stabilization • Goal is to initiate movement with the upper extremities in a pushup pattern without allowing movement in the spine or hips. • Extension and rotation are the two most common compensatory movements. These compensations indicate the prime movers within the pushup incorrectly engage before the stabilizers. • Test the ability to stabilize the spine in the sagittal plane. • Men with thumbs at the top of the forehead • Women with thumbs at chin level.
Implications • Limited performance during the test can be attributed to poor reflex stabilization of the core • Compromised upper body strength or scapular stability – or both- an also be a cause of poor performance • Limited hip and thoracic spine mobility can affect an clients ability to achieve the optimal start position, also leading to poor performance. • Clearing exam- extension (cobra)
Rotary Stability Pattern • Observes multi-plane pelvis, core and shoulder girdle stability during a combined upper and lower extremity movement. • Demonstrates reflex stabilization and weight shifting in the transverse plane, and represents the coordinated efforts of mobility and stability observed in fundamental climbing patterns. • Implications in compromised scapular and hip stability • Limited knee, hip, spine, and shoulder mobility.