Future Directions in HCV Therapy: Insights and Milestones in Treatment
630 likes | 767 Vues
This presentation by Dr. Eric Lawitz discusses the evolution of chronic hepatitis C therapy, detailing advancements that have led to higher sustained virologic response (SVR) rates with the introduction of direct-acting antivirals (DAAs). It highlights key studies, including NEUTRINO, FISSION, and POSITRON, unveiling the efficacy and safety profiles of treatment regimens, particularly focusing on patients with difficult-to-treat conditions. The talk emphasizes current limitations in the therapy landscape and paves the way for future innovations in HCV management.

Future Directions in HCV Therapy: Insights and Milestones in Treatment
E N D
Presentation Transcript
Future Directions in HCV Therapy Eric Lawitz, MD, AGAF,CPI Medical Director, The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center San Antonio, Texas
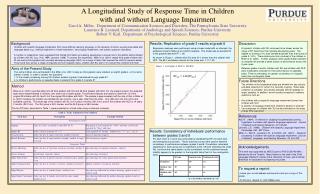
Milestones in Therapy of CHC:Average SVR Rates from Clinical Trials + DAAs Peginterferon 2011 2001 + Ribavirin Standard Interferon 1998 70+% 1991 55% 42% 39% 34% 16% 6% Adapted from US Food and Drug Administration, Antiviral Drugs Advisory Committee Meeting, April 27-28, 2011, Silver Spring MD.
DAAs with an Indication for the Treatment of G1 Chronic Hepatitis C • Both compounds act by inhibiting HCV nonstructural NS3/4A protease and are referred to as direct acting antivirals (DAAs) US Food and Drug Administration. Available at http://www.accessdata.fda.gov/scripts/cder/drugsatfda/
Limitations of Current Therapy • Telaprevir and boceprevir only approved for Genotype 1 • Interferon backbone required • TID dosing for telaprevir/boceprevir • Response guided therapy (both) and lead-in (boceprevir) complicated • 24-48 week treatment • Limited efficacy in difficult to cure patients (e.g., patients with cirrhosis, prior null responders, African-Americans) • Hematologic (both) and rash/dermatological (telaprevir) adverse events • Drug-drug interactions
Sofosbuvir (SOF) (GS-7977) • NS5B nucleotide polymerase inhibitor • Favorable administration profile • Once daily, no food effect • No drug-drug interactions
Completed Phase 3 Trials • NEUTRINO • GT 1, 4, 5, 6; treatment naïve • No comparator • FISSION • GT 2 and 3; treatment naïve • Compared to 24 weeks of peginterferon + ribavirin • POSITRON • GT 2 and 3; patients ineligible for or intolerant of interferon therapy • Compared to placebo • FUSION • GT 2 and 3; patients unresponsive to prior treatment • Compared to 16 weeks of sofosbuvir + ribavirin
NEUTRINO • Patients • GT 1, 4, 5, 6 treatment naive • 17% compensated cirrhosis • 17% black • 29% IL28B genotype CC • Regimen for all patients • Sofosbuvir 400 mg qd • Ribavirin 1000/1200 mg qd • Peginterferon alfa-2a 180 mcg weekly E. Lawitz et al, Abstract 1411. EASL, April 2013; Lawitz et al., N Engl J Med 2013, 368: 1878-1887.
NEUTRINO: Study Design Week 0 12 24 • Open label • SOF+PEG+RBV for 12 weeks (no response-guided therapy) • Expanded inclusion criteria • No upper limit to age or BMI • Opiate replacement therapy permitted • Platelets ≥90,000/mm3, neutrophils ≥1,500/mm3or1,000/mm3 (blacks) SVR12 Sofosbuvir/PEG/RBV, n=327 E. Lawitz et al, Abstract 1411. EASL, April 2013; Lawitz et al., N Engl J Med 2013, 368: 1878-1887.
>90% Of Patients Have Undetectable Virus After 2 Weeks and Achieve SVR 326/327 321/325 299/327 295/327 Week 12 Week 2 Week 4 Week 12 Post-treatment On treatment E. Lawitz et al, Abstract 1411. EASL, April 2013; Lawitz et al., N Engl J Med 2013, 368: 1878-1887.
NEUTRINO: SVR by Genotype n = 292 n = 7 n = 28 295/327 261/292 27/28 7/7 E. Lawitz et al, Abstract 1411. EASL, April 2013; Lawitz et al., N Engl J Med 2013, 368: 1878-1887.
NEUTRINO: SVR by Subgroup n = 273 n = 54 n = 95 n = 54 n = 95 n = 232 n = 54 n = 273 n = 54 Black No cirrhosis Cirrhosis CC CT/TT IL28B genotype E. Lawitz et al, Abstract 1411. EASL, April 2013; Lawitz et al., N Engl J Med 2013, 368: 1878-1887.
Conclusions • 12 weeks of SOF+PEG+RBV achieved 90% SVR in treatment naïve patients with GT 1, 4, 5, or 6 • 99% of patients had HCV RNA < LLOQ by treatment week 4 and all virologic failures were due to relapse • This regimen was well tolerated E. Lawitz et al, Abstract 1411. EASL, April 2013; Lawitz et al., N Engl J Med 2013, 368: 1878-1887.
GT2 and GT 3: Study Designs FISSION (TN) Week 0 12 24 Week 0 12 24 36 SVR12 SVR12 SOF + RBV, n=256 SOF + RBV, n=207 SVR12 Placebo SOF + RBV, n=103 RBV does 1000-1200 mg/day for SOF + RBV and 800 mg/day for Peg-IFN + RBV. SVR12 SVR12 Peg-IFN + RBV (SOC), n=243 SOF + RBV, n=98 FUSION (TE) SVR12 Placebo, n=71 Week 0 12 16 24 28 SOF dose 400 mg once daily; RBV dose 1000-1200 mg/day. POSITRON (Intolerant) SOF dose 400 mg once daily; RBV dose 1000-1200 mg/day. Jacobson et al. N Engl J Med 2013, 368: 1867-1877, Lawitz et al., N Engl J Med 2013, 368: 1878-1887,
GT2 and GT 3: SVR by Genotype FISSION (TN) 97 78 63 67 67 56 SVR12 (%) 68/70 52/67 170/253 162/243 102/183 110/176 P <0.001 P <0.001 FUSION (TE) 94 86 73 62 50 30 SVR12 (%) 31/36 30/32 69/95 39/63 50/100 19/64 POSITRON (Intolerant) 93 78 61 SOF + RBV 12 weeks SVR12 (%) 161/207 101/109 60/98 Jacobson et al. N Engl J Med 2013, 368: 1867-1877, Lawitz et al., N Engl J Med 2013, 368: 1878-1887,
SVR: Patients with CirrhosisvsNo Cirrhosis FISSION (TN) 98 91 82 71 61 62 34 30 SVR12 (%) 10/11 58/59 44/54 89/145 99/139 8/13 11/37 13/38 GT 2 GT 3 FUSION (TE) 100 96 61 78 63 60 37 19 SVR12 (%) 14/23 25/40 25/26 23/23 14/38 5/26 6/10 7/9 GT 2 GT 3 POSITRON (Intolerant) 92 94 68 SVR12 (%) 21 85/92 16/17 67/84 3/14 Jacobson et al. N Engl J Med 2013, 368: 1867-1877, Lawitz et al., N Engl J Med 2013, 368: 1878-1887,
Conclusions • 12 weeks of SOF+RBV results in SVR>90% in GT 2 treatment naive patients with and without cirrhosis • SVR rates were lower in GT 2 treatment experienced patients with cirrhosis compared to non-cirrhosis • SOF+RBV led to similar results as PEG+RBV for GT 3 treatment naïve patients • Lowest rates observed in patients with cirrhosis • SOF+RBV for 12 weeks is suboptimal for GT 3 treatment experienced patients • 16 weeks total duration significantly increased SVR rates • SOF+RBV well tolerated with fewer adverse events than PEG+RBV • Genotype 3 ≠ genotype 2 HCV • Strategies to improve GT 3 results are needed
Simeprevir (TMC 435) • NS3/4A protease inhibitor • Antiviral activity against GT 1, 2, 4, 5 and 6 • One capsule, once per day
Completed Phase 3 Studies • QUEST-1 and QUEST-2 • Same study design but studies conducted independent of one another • Treatment naïve GT 1 patients • PROMISE • Same study design as QUEST-1 and QUEST-2 • GT 1 prior relapsers
QUEST-1, QUEST-2 andPROMISE Study Designs Response Guided Treatment • Response Guided Therapy: if HCV RNA <25 IU/mL at Week 4 and undetectable at Week 12, complete treatment at Week 24 • 85-93% of patients met the criteria and qualified for total treatment duration of 24 weeks. Post-Therapy Follow-Up Post-Therapy Follow-Up Placebo/ PEG/RBV SMV 150 mg/PEG/RBV PEG/RBV PEG/RBV PEG/RBV PEG/RBV Post-Therapy Follow-Up Weeks 0 24 12 48 72
Simeprevir + PEG/RBV Achieved SVR in ~80% of Treatment Naïve and Prior Relapsers 81% 80% 79% 50% 50% 37%
QUEST-1: SVR by Subgroup 152/ 183 54/ 90 54/ 77 11/ 40 105/ 147 36/ 74 105/ 117 29/ 56 72/ 77 29/ 37 114/ 150 32/ 76 24/ 37 4/ 17 Fibrosis Genotype IL28B genotype I. Jacobson et al, Abstract 1425. EASL, April 2013
SVR Higher When SimeprevirAdded to PEG/RBV For Patients With All Stages of Fibrosis/Cirrhosis (QUEST-2) 165/ 195 52/ 102 24/ 36 9/ 17 11/ 17 6/ 15 F0-F2 F3 F4 (Cirrhosis) Similar results seen in QUEST-1 and PROMISE studies
Conclusions • Simeprevir150 mg + PEG/RBV was highly effective against GT 1 treatment naïve patients with SVR (80%) • Most patients (85%) receiving simeprevirwere able to shorten therapy to 24 weeks • Simeprevir150 mg + PEG/RBV was generally well tolerated • Rates of anemia and rash were similar in the simeprevir and placebo groups I. Jacobson et al, Abstract 1425. EASL, April 2013
COSMOS: Study Design n = 24 Post-treatmentfollow-up SMV + SOF + RBV Arm 1 n = 15 SMV + SOF Post-treatmentfollow-up Arm 2 SMV + SOF + RBV n = 27 Arm 3 Post-treatment follow-up • Cohort 1: n=80patients randomized 2:1:2:1 • Cohort 2: n=87 patients randomized 2:1:2:1 • SMV 150 mg QD + SOF 400 mg QD with/without RBV (Copegus®) 1000 or 1200 mg/day (BID) • Interim analysis of Cohort 1 conducted when all patients in 12 week treatment arms (arms 3 and 4) reached SVR4 time point or discontinued early SMV+ SOF Arm 4 n = 14 Post-treatment follow-up Weeks 0 12 24 36 48 Interim analysis SVR4 Primary endpoint SVR12 Lawitz et al., CROI, March 2013
COSMOS: Key Eligibility Criteria –Cohort 1 • Chronic HCV GT 1 infection • 78% GT 1a • Prior null response to PEG/RBV • Failure to achieve >2 log10 decline in HCV RNA by Week 12 • Fibrosis • F0-F1: 41% • F2: 59% • IL28B • CT: 70% • TT: 24% • 29% African-American Lawitz et al., CROI, March 2013
COSMOS: Virologic Response (12 Week Arms) SVR8 (%) 23/27 8/14 27/27 14/14 26/27 13/14 26/27 13/14 • RVR, n/N (%) • Undetectable end of treatment, n/N (%) • SVR4, n/N (%) • SVR8, n/N (%) Lawitz et al., CROI, March 2013
COSMOS: Safety & Tolerability 1WHO Toxicity Grading Scale, 2003 Lawitz et al., CROI, March 2013
COSMOS: Cohort 2 • SMV+SOF+RBV for 12 weeks • GT 1 treatment naive and prior null responders with advanced disease (F3/F4) • SVR4 results • SMV+SOF+RBV: 96% (26/27) • SMV+SOF: 100% (14/14) Medivir/Janssen Press Release, August 29, 2013
COSMOS: Summary • 12 weeks of SMV+SOF led to an SVR8 rate of 96% with RBV and 93% without RBV in prior null responders with F0-F2 disease • 12 weeks of SMV+SOF led to an SVR4 rate of 96% with RBV and 100% without RBV in treatment naïve and prior null responders with F3-F4 disease • SMV+SOF+RBV was generally well tolerated
Background • Patients who experience virologic failure on telaprevir or boceprevir-based regimens currently have no treatment options • DCV plus SOF with or without RBV achieved SVR4 in 98% of 126 HCV GT 1-infected treatment-naive patients (Sulkowski et al. AASLD 2012) • Study Aim • To evaluate the efficacy and safety of DCV+SOF with or without RBV for 24 weeks in GT 1-infected patients who failed prior treatment with TVR or BOC + PEG/RBV M.S. Sulkowski et al, Abstract 1417. EASL, April 2013
Study Design Follow-up n = 21 • Patients • GT 1, non-cirrhotic • Prior nonresponse, relapse, or breakthrough during treatment with PEG/RBV+TVR or BOC • Patients who discontinued TVR or BOC due to an AE were excluded • DCV 60 mg QD + SOF 400 mg QD Prior TVR/BOC Failures, GT 1a/1b (N = 41) Follow-up • DCV 60 mg QD + SOF 400 mg QD + RBV n = 20 SVR12 Week 24 SVR4 M.S. Sulkowski et al, Abstract 1417. EASL, April 2013
Virologic Response • 1 patient missing at post-treatment (PT) Week 12: HCV RNA was undetectable at PT Week 4 and at PT Week 24 • 21/41 patients have reached PT Week 24; all have achieved SVR24 DCV + SOF + RBV DCV + SOF HCV RNA < LLOQ (% patients) Missing N = 21 20 21 20 21 20 21 20 21 20 EOT Week 2 Week 4 SVR4 SVR12 M.S. Sulkowski et al, Abstract 1417. EASL, April 2013
Conclusions • The all-oral, once-daily combination of DCV+SOF with or without RBV achieved SVR in all GT 1 infected patients (n=41) who failed prior treatment with TVR or BOC+PEG/RBV • DCV+SOF with or without RBV waswell tolerated • No Grade 3 or 4 hepatic or hematologic abnormalities M.S. Sulkowski et al, Abstract 1417. EASL, April 2013
Daclatasvir (BMS-790062) (NS5A inhibitor) + Asunaprevir (BMS-650032) (PI)
Study AI447-011 Expansion Cohort:Prior Null Responders to PEG/RBV Week 24 SVR12 primary endpoint SVR48 Follow-up A1 (DUAL): DCV 60 mg QD + ASV 200 mg BID (GT 1b only) A2 (DUAL): DCV 60 mg QD + ASV 200 mg QD (GT 1b only) Follow-up N = 18 Follow-up B1 (QUAD): DCV 60 mg QD + ASV 200 mg BID + PEG/RBV (GT 1a/1b) Follow-up B2 (QUAD): DCV 60 mg QD + ASV 200 mg QD + PEG/RBV (GT 1a/1b) N = 20 B3 (TRIPLE): DCV 60 mg QD + ASV 200 mg BID + RBV (GT 1a/1b) Follow-up N = 20 N = 21 N = 22 SVR4 SVR24 Week 12 A. Lok, et al; APASL 2013.
TRIPLE Therapy (Arm B3): GT 1a vs GT 1bIndividual HCV RNA Levels • 1/18 GT 1a patient completed triple therapy and achieved SVR4 DCV + ASV 200 mg BID + RBV Graphs truncated at viral breakthrough LLOQ LLOQ LOD LOD
Conclusions • In non-cirrhotic prior null responders,24 weeks of daclatasvir + asunaprevir appears to be an efficacious combination for GT 1b but not GT 1a
Daclatasvir (BMS-790062) (NS5A inhibitor) + Asunaprevir (BMS-650032) (PI) + BMS-791325 (non-nuc)
AI443-014: Study Design • Treatment naïve non-cirrhotic patients • GT 1a: 74% and CT/TT: 70% G. Everson et al, Abstract 1423. EASL, April 2013
Summary The all oral, IFN-free, RBV-free, ritonavir-free combination of DCV, ASV, and BMS-791325 • Achieved >90% (61/66) SVR4 and SVR12 (30/32) • Had infrequent virologic failure (4.5%, 3/66) • Most common AEs (≥10% total) were headache, asthenia, and gastrointestinal G. Everson et al, Abstract 1423. EASL, April 2013
Faldaprevir: Phase 3 Studies (IFN-Containing) • STARTVerso1 • Treatment naïve GT 1 patients • All patients from Europe and Japan • Only Phase 3 study with results reported as of October 2013 • STARTVerso 2 • Treatment naïve GT 1 patients • Studying shorter durations (12 vs 24 weeks) • STARTVerso3 • Treatment experienced GT 1 patients • STARTVerso4 • Treatment naïve/prior relapsers who are coinfected with HCV and HIV
STARTVerso1 • Phase III, randomized, double-blind, placebo-controlled trial • Patients • Treatment naïve GT 1 infection • 78% Caucasian, 20% Asian • 39% IL28B CC • 66% GT 1b • Regimen • PEG+RBV for 24 weeks plus faldaprevir/placebo • Patients with early treatment success stopped all treatment atWeek 24 • Patients without Early Treatment Success and those in control arm received PEG/RBV for 48 weeks P. Ferenci et al, Abstract 1416. EASL, April 2013
PBO/PEG/RBV PEG/RBV Observation Period STARTVerso1: Study Design • Criteria for response guided therapy • Early Treatment Success (ETS): HCV RNA <25 IU/mL at Week 4 and undetectable at Week 12, complete treatment at Week 24 • 88% met the criteria and qualified for total treatment duration of 24 weeks. Observation Period ETS FDV240 mg/PEG/RBV PBO/ PEG/RBV PEG/RBV Observation Period No ETS PBO/ PEG/RBV Observation Period ETS FDV 120 mg/ PEG/RBV Observation Period FDV 120 mg/ PEG/RBV PEG/RBV No ETS Day 1 Week 12 Week 24 Week 48 Week 72 P. Ferenci et al, Abstract 1416. EASL, April 2013
STARTVerso1 SVR12 rates 69 132 210 261 204 259 P. Ferenci et al, Abstract 1416. EASL, April 2013
SVR in Patients With Cirrhosis 195/243 204/246 9/16 6/15 FDV 120 mg/ PEG/RBV FDV 240 mg/ PEG/RBV FDV 120 mg/ PEG/RBV FDV 240 mg/ PEG/RBV No Cirrhosis Cirrhosis P. Ferenci et al, Abstract 1416. EASL, April 2013
SVR By GT 1 Subtype 16/45 60/87 68/90 52/86 143/171 142/171 FDV 120 mg/ PEG/RBV FDV 240 mg/ PEG/RBV PEG/RBV FDV 120 mg/ PEG/RBV FDV 240 mg/ PEG/RBV PEG/RBV GT1a GT1b P. Ferenci et al, Abstract 1416. EASL, April 2013