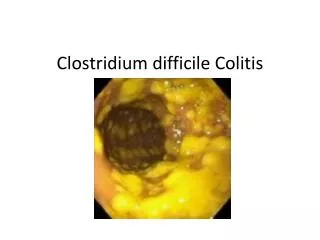
Infectious Disease Lecture Series - C. Difficile colitis John Pullman MD F.A.C.P.
Infectious Disease Lecture Series - C. Difficile colitis John Pullman MD F.A.C.P. Excerpted from: Epidemiology, Pathogenesis, Diagnosis and Treatment of Clostridium difficile Infection (CDI) Courtesy of Dale N. Gerding, MD Professor of Medicine

Infectious Disease Lecture Series - C. Difficile colitis John Pullman MD F.A.C.P.
E N D
Presentation Transcript
Infectious Disease Lecture Series - C. Difficile colitisJohn Pullman MD F.A.C.P. Excerpted from: Epidemiology, Pathogenesis, Diagnosis and Treatment of Clostridium difficile Infection (CDI) Courtesy of Dale N. Gerding, MD Professor of Medicine Loyola University Chicago Stritch School of Medicine Associate Chief of Staff for Research Hines VA Hospital
Written Disclosures Objectives At the end of this continuing nursing education event, participants should be able to: • Describe the natural history of C. Difficile colitis. • Describe the rationale for current treatment guidelines. • Describe the challenges in the diagnosis and management of C. Difficile colitis. • Differentiate the contribution and coordination of patient care delivery team members: nursing, laboratory services, pharmacy and physician. Criteria for Successful Completion: • Viewing 100% of the video-taped educational event. • Completion of the Independent Study Evaluation Form.
Written Disclosures - continued Disclosure of presenter: John Pullman MD F.A.C.P. discloses that he receives Grant/Research Support from Sanofi Aventis, Optimer, Merck and Genzyme. Disclosure of those in a position to control educational content: Phil Dean RN, Clinical Nurse Educator has nothing to disclose. Enduring Material for Independent Study Expires: 3/29/14
C. difficile (CDI) Update • The 2000s have been characterized by a completely unanticipated CDI epidemic in North America and Europe through 2010. • The epidemic is due in part to the BI/NAP1/027 strain now found in 30%-40% of randomized CDI cases in North America. • CDI diagnosis remains an enigma. • Vancomycin is superior to metronidazole for severe CDI in 2 of 3 randomized trials. • Fidaxomicin (OPT-80) and monoclonal anti-bodies significantly reduce CDI recurrence.
National Estimates of US Short-Stay Hospital Discharges With C. difficile as First-Listed or Any Diagnosis, National Inpatient Sample 400,000 350,000 Any listed Primary 300,000 250,000 Number of Discharges 200,000 150,000 100,000 50,000 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 Year Elixhauser A, Jhung MA. Clostridium difficile–associated disease in U.S. hospitals, 1993–2005. HCUP Statistical Brief #50. April 2008. Agency for Healthcare Research and Quality, Rockville, MD and unpublished data http://www.hcup-us.ahrq.gov/reports/statbriefs/sb50.pdf.
CDI Public Reporting: Ohio 2006 • 14,329 primary and recurrent CDI cases • 210 Acute Care Hospitals • ~5,217 primary cases; 6.4-8 per 10,000 patient-days • ~1,159 recurrent cases; 1-2 per 10,000 patient-days • ~6,376 total CDI cases reported by acute hospitals • 955 Nursing Homes (Long-term Care Facilities) • ~4,880 primary cases; 1.7-2.9 per 10,000 patient-days • ~3,073 recurrent cases; 1-2 per 10,000 patient-days • ~7,953 total CDI cases reported by Nursing Homes • Are Ohio Nursing Homes representative of CDI rates nationally? Campbell RJ et al Inf Control Hosp Epidemiol 2009;30:526-533
TYPING SYSTEMS/ NOMENCLATURE FOR THE RECENT EPIDEMIC C. difficile STRAIN Toxinotype [Epidemic strain: III] (Rupnik) Slovenia, EU; Characterization of toxin gene variations based on PCR-RFLP analysis of the pathogenicity locus (PaLoc) PCR Ribotype [Epidemic strain: 027] (Brazier) Wales, UK; CD isolate collection > 9,000 isolates REA [Epidemic strain: Group BI (Bee-Eye)] (Gerding) Chicago, US; CD isolate collection > 8,000 isolates PFGE [Epidemic strain: NAP-1] (McDonald-Killgore) Atlanta, US; CDC initiated surveillance for CD in 2004
Current Epidemic Strain of C. difficile • BI/NAP1/027, toxinotype III • Historically uncommon and without high-level resistance to fluoroquinolones • Epidemic since 2000 • Epidemic behavior coincident with increased resistance to fluoroquinolones • Carries extra toxin known as binary toxin • Clearly more virulent: mechanisms? • High toxin A and B production in vitro • Polymorphisms in binding domain of toxin B • Increased sporulation McDonald LC et al. N Engl J Med. 2005;353:2433.Warny M et al. Lancet. 2005;366:1079. Stabler RA et al. J Med Micro. 2008;57:771. Akerlund T et al. J Clin Microbiol. 2008;46:1530.
States with BI/NAP1/027 strain of C. difficile (N=40), October, 2008 West 32% East 60% Midwest 62% DC HI PR AK CDC and Cheknis et al ICAAC San Francisco 2009
Percent NAP1/BI C. difficile Isolates in Canadian Provinces in 2005 Alberta BC 20% 12% Sask/Man Quebec Atlantic Provinces Ontario 7% 76% 5% 22% IDSA-ICAAC 2008, Miller M, Canadian Nosocomial Infection Surveillance Program (CNISP).
Recent Surveys of Clinical C. difficile Isolates in North America and Europe • Voluntary specimen submission (2006 to 2009) - Cd isolates from stool specimens submitted by hospitals throughout the U.S. to obtain current CDI epidemiology Cheknis ICAAC 2009 REAPCR riboUS N REA Typing results: BI 027 54% (296/548) Y 014,020 8% (43/548) J 001 4% (20/548) • Tolevamer Study (2005 to 2007) - Cd isolates from Phase III Multi-center, NA and EU CDI Trials Cheknis ICAAC 2007REAPCR riboNA StudyNEU Study REA Typing results: BI 027 36% (138/398)8% J 001 12% (48/398) 18% Y 6,14,20 9% (36/398) 14% • Fidaxomicin Study (2006 to 2010) -Cd isolates from Phase III Multi-center, NA and EU CDI Trial Gerding ICAAC 2010 REAPCR riboNA/EUN REA Typing results: BI 027 34% (244/716) Y 014,020 11% (77/716) G 002 8% (54/716)
Nominal Differences in Strain Type Between Community- and Health Care–Associated C. difficile Community-associated NAP1 NAP1 related Health care–associated NAP2 NAP4 NAP5 NAP6 All NAP7 NAP10 NAP11 unnamed Slide courtesy Cliff McDonald and CDC *Unnamed group consists of 26 unique PFGE types Dumyati G et al IDSA 2009, Philadelphia; Thompson AD et al ICAAC2009 San Francisco; Abstract K-2071.
Case Review A 67 yr old man with COPD and CAP develops watery stools on his third day on the pneumonia protocol. He has 3-4 BMs in a 5 hour period and is incontinent of stool. Stool study for C difficile toxin assay is pending (otherwise known as “waitin’ on the night shift”). What findings warrant empiric treatment to be ordered? What determines isolation precautions? When instituted, can they be ever be discontinued before discharge? His stool assay may be reported ‘negative’. What are the causes for a false-negative assay?
Clostridium difficile Hospital Epidemiology • Use of Antibiotics is frequent (and often inappropriate) • Environmental contamination by C. difficile is common (spores difficult to eradicate) • Personnel carry C. difficile on their hands • Asymptomatic and infected patients carry C. difficile and can contaminate the environment • Hospitalized patients are older
Host Protection Against CDI Occurs at Two Levels • Normal bacterial flora prevent establishment of C. difficile colonization of the GI tract • Serum (and mucosal?) antibodies prevent CDI if colonization occurs • Antibodies probably first acquired in infancy
Current Pathogenesis Model for C. difficile Infection (CDI) C. difficile acquisition C. difficile acquisition Asymptomatic C. difficile colonization Antimicrobial(s) CDI Hospitalization Acquisition of a toxigenic strain of C. difficile and failure to mount an anamnestic Toxin A IgG antibody response results in CDI. Kyne et al NEJM 2000
Rate of C. difficile Acquisition in Hospitalized Patients as Determined by Weekly Rectal Swab Cultures 50 40 C. difficile 30 Percentage of Patients who 20 Acquired 10 0 0 1 2 3 4 >4 <1 3-4 1-2 2-3 Length of hospital stay (w) Ref: Johnson and Gerding Clin Infect Dis 1998;26:102-7
C. difficile in the Environment • 2580 environmental samples from Cardiff area of Wales • 7.1% of all samples positive for C. difficile • River water samples 87.5% positive • Swimming pools 50% positive • Lake water 47% positive • Sea water samples (beaches) 44% positive • Soil samples 21% positive • Tap water 6% positive • Dog feces 10% positive • Cat feces 2% positive • Home environments 2.2% positive • Raw vegetables 2.4% positive (Vegetarians take note) • Ready-to-eat salads 7.5% positive (Vegetarians take note) • Farm animal feces 1% positive (Carnivores take heart) • Fish guts 0% positive (Is there hope for a safe food source?) al Saif and Brazier J Med Micro 1996;45:133, Bakri et al EID 2009;15:817
Role of Antibiotics in Clostridium difficile Infection (CDI) • Any antibiotic may be associated with CDI. • Disruption of normal intestinal flora is likely the determining antibiotic event. (anaerobic activity?) • C. difficile resistance to the precipitating antibiotic is thought to be important, but is not always present (e.g. ampicillin).
Time-Course of Antimicrobial Effect on the Normal Gut Flora and CDI Risk Antibiotic Use NO Antibiotics NO Antibiotics NO Antibiotics Flora Disrupted Normal Flora Normal Flora Flora Disrupted CDI Risk Arrows indicate variable time Flora Depressed C. difficile that is resistant to the antibiotic has a selective advantage Resistant or susceptible C. difficile has an equal advantage No CDI risk No CDI risk
Before Testing • Be certain that the population being tested has symptoms consistent with CDI. The stool should be watery or unformed (and should be rejected by the microbiology laboratory for testing if it is not) and the patient should meet minimum clinical criteria for diarrhea (>3 loose or unformed stools in 24h or less).
Key Problem: CDI Diagnosis • Standard Reference Tests: Cell cytotoxicity and Toxigenic Culture – both too slow • Enzyme immunoassays are insensitive • Test Sensitivity, Specificity, and Turnaround Time are critical to improved testing • Two-Step GDH: Too insensitive and too slow? • Poor sensitivity cannot be overcome by sending more specimens – No Cdiff X 3!!! • RT-PCR for CDI diagnosis is likely one good answer to the diagnosis problem.
SHEA/IDSA CDI Guideline: Diagnosis Recommendations • Sensitivity and specificity of a stool culture and identification of a toxigenic isolate (ie, toxigenic culture)… “provides the standard against which other clinical test results should be compared” (B-III) • “EIA testing for… toxin A and B is rapid but is less sensitive than the cell cytotoxin assay and is thus …suboptimal” (B-II) • “Toxin testing is most important clinically, but is hampered by the lack of sensitivity.” One potential strategy to overcome this problem is a 2-step method using EIA for GDH as an initial screen and the cell cytotoxicity assay or toxigenic culture as the confirmatory test only on GDH positive stools (B-II) Cohen SH et al. Infect Control Hosp Epidemiol. 2010;31:431.
Diagnosis Recommendations • “PCR testing appears to be rapid, sensitive and specific and may ultimately address testing concerns.” More data needed (B-II) • “Repeat testing during the same episode of diarrhea is of limited value and should be discouraged” (B-II) Interpretation: “No more C. diff X 3” Cohen SH et al. Infect Control Hosp Epidemiol. 2010;31:431.
Can Low Test Sensitivity be Overcome by Repeated Testing? It Depends upon the Specificity. 1000 Tests with 10% CDI Prevalence in Population Sensitivity= 73.3% Specificity = 97.6% For typical EIA sensitivity and specificity, false positives exceed true positives with repeated testing. Peterson LR, Robicsek A. Ann Intern Med. 2009;151:176-179
RT-PCR vs Toxigenic Culture using Commercial RT-PCR PPV = Positive Predictive Value, NPV = Negative Predictive Value Barbut F et al and Loo V et al ICAAC-IDSA 2008, Washington DC Abstracts D-2279 and D-2281
Unresolved CDI Diagnosis Issues • Slow turnaround of the most sensitive current tests (cell cytotoxicity, culture) • Use of a two-step GDH-EIA still results in slow turnaround for positive test results unless PCR is used as the confirmatory test, and may not be sufficiently sensitive as a screening test compared to RT-PCR. • RT-PCR appears to be the most sensitive and rapid test, but it is more costly. • Is gene detection by RT-PCR equivalent to toxin detection for diagnosis of CDI?
Case Review At 11:55 PM, Jackie (RN) calls with the report of a watery stool on an 87 yr old woman recovering from ORIF of a closed hip fracture 5 days ago. She (ever-vigilant) has saved a specimen and informs you that it ‘smells like C diff’! What two questions must you ask before you cave in to her request to send the stool for a C diff assay? What other bits of information can you glean to decide, at that point, to initiate Rx: which one and how much and how long? After 10 days of successful Rx, her daughter wants a repeat stool for C diff toxin “to be sure Mum’s cleared up! What’s your firm but calm reply?
Case Review • A 46 yr old petroleum engineer returns from Nigeria after a 6 month stay in an inland compound. He gives a history of an episode of traveller’s diarrhea 6 weeks after arrival that responded to 3 days of cipro 500 mg 3x daily. Now he has had watery diarrhea >10x daily for 8 days despite a repeat course of cipro the first three days of recurrent symptoms and his stool is bloody. • What stool tests do you consider, given his travel history alone? Especially if he gives a history of fever, what other lab tests are warranted? • What empiric therapy would be best pending reports?
Case Review • A 22 yr old man presents with a history of watery stools >3 x daily for three days. He has no fever, abdominal cramps, blood in the stools. No household contacts have had any similar symptoms. • What stool studies are indicated? • Are there points in his history that might change you mind regarding what, if any studies, are indicated? • Is there an argument for empiric antibiotic treatment pending the results of any of these studies? What would that Rx be and what would it treat?
Case Review A 34 yr old woman working at an animal shelter with others were overwhelmed with 100+ dogs, many of whom were pregnant, when an animal hoarder’s bus broke down on a highway in BSB County. They all had severe malnutrition and especially with re-feeding, developed an overwhelming diarrhea. Crowding was unavoidable and control of feces difficult. (It flew frequently across the cages and rooms; the staff were outnumbered and out-gunned and seriously short of defense items…) 3 workers developed watery diarrhea + Campylobacter jejeuni. What antibiotic was indicated? What neurological complication of the infection occurred and why ?
Current Treatment Summary • Treatment of first episode CDI is unchanged in 30 years • Stop offending antibiotics if at all possible –effective in 25% of patients with no other treatment and if antibiotics are continued the success of CDI treatment is less likely. • Treat with metronidazole (mild CDI) or • Treat with vancomycin (severe CDI)
Treatment Recommendations • “Metronidazole is the drug of choice for the initial episode of mild-moderate CDI” (500 mg orally TID) for 10–14 days (A-I) • “Vancomycin is the drug of choice for an initial episode of severe CDI”. The dose is 125 mg orally QID for 10–14 days (B-I) Cohen SH et al. Infect Control Hosp Epidemiol. 2010;31:431.
No Validated Definition of Severity • Zar FA et al. Clin Infect Dis. 2007;45:302. • PMC, treatment in ICU, or 2 of the following: • Age >60, temp >38.3°C, albumin <2.5/dL, WBC >15,000/mm3 • Louie T et al ICAAC; Chicago 2007; Abstract 3826. • ≥10 bowel movements/day or • WBC >20,000/mm3 or • Severe abdominal pain • Cohen SH et al. Infect Control Hosp Epidemiol.2010;31:431.* • WBC >15,000/mm3 or • Creatinine > 1.5× baseline *2010 SHEA/IDSA Guidelines
Response to CDI Treatment when Stratified by Disease Severity Clinical Cure in Mild Disease (n=81) Clinical Cure in Severe Disease* (n=69) P=0.36 P=0.02 98 100 100 97 90 90 90 76 80 80 70 70 39/40 30/31 37/41 29/38 60 60 50 50 Percent of Patients Percent of Patients 40 40 30 30 20 20 10 10 0 0 Metronidazole Vancomycin Metronidazole Vancomycin *Severe disease defined as intensive care unit admission; pseudomembranous colitis on endoscopy;or at least two of the following: 1) Age >60 years, 2) Temperature >101°F, 3) Albumin level <2.5 mg/dL, 4) White blood cell count (WBC) >15,000 cells/mm3 Zar FA, et al. Clin Infect Dis. 2007;45:302-307.
Response to Treatment in Controlled Trials Tolevamer Phase III North American data 85% 85% P=0.04 80% 79% P=.04 76% 65% 59% Clinical Success 46% 37% * † ‡ * 3–5 BM/d or WBC ≤15,000/mm3or mild abdominal pain due to CDI. † 6–9 BM/d orWBC 15,000–20,000/mm3ormoderate abdominal pain due to CDI. ‡ ≥10 BM/d or WBC >20,000/mm3or severe abdominal pain due to CDI. Louie T, et al. ICAAC 2007. Abstract K-425-a.
Effect of Continued Concomitant Antibiotics on Treatment of CDI • Prospective randomized double blind trial of vancomycin vs. fidaxomicin in 548 patients with CDI. • Antibiotics discontinued in 409 but continued in 89 patients. • Combined data for vancomycin and fidaxomicin shown in the table. Mullane KM et al, IDSA 2009, Philadelphia 2009
Treatment Recommendations:Severe, Complicated CDI(Hypotension or Shock, Ileus, Megacolon) • Vancomycin orally (and per rectum if ileus is present) with or without metronidazole IV for severe, complicated CDI. Vancomycin is dosed at 500 mg (C-III) • “Consider colectomy for severely ill patients” (ideally before) serum lactate rises to 5 mmol/L and WBC to 50,000 per uL (B-II) Cohen SH et al. Infect Control Hosp Epidemiol. 2010;31:431.
Unresolved Issues in Treatmentof Severe, Complicated CDI • Evidence for antibiotic treatment recommendations (including vancomycin dosing at 500 mg) is poor and anecdotal (eg, C-III) • Potential adjunctive/alternative treatments: • IV tigecycline in place of IV metronidazole1 • IVIG2 • Monoclonal antibodies against CD toxins3 • 1. Herpers BL et al. Clin Infect Dis. 2009;48:1732. • 2. Abougergi MS et al. J Hosp Med. 2010;5:E1. • 3. Lowy I et al. N Engl J Med. 2010;362:197.
Treatment Recommendations: Recurrent CDI • “Treatment of the first recurrence is usually with the same regimen as for the initial episode (A-II) but should be stratified by disease severity…”(C-III) (Recurrence is a host problem, not an antimicrobial treatment failure problem.) • “Do not use metronidazole beyond the first recurrence... or for long-term chronic therapy” (B-II) • “Treatment of the second or later recurrence with vancomycin using a tapered and/or pulse regimen is the preferred next strategy” (B-III) • “No recommendations can be made regarding prevention of recurrent CDI in patients who require continued antimicrobial therapy…” (C-III) Cohen SH et al. Infect Control Hosp Epidemiol. 2010;31:431.
Treatment Strategies for 163 Cases of Recurrent C. difficile Disease that were Controls in S. boulardii Trials *P<.05 compared to medium dose vancomycin (Lane 1) * 1g/d .5g/d 2g/d N=14 N=48 N=21 N=29 * Taper N=7 Pulse Vancomycin Metronidazole (Various doses) McFarland et al. Am J Gastroenterol 2002;97:1769-1775
Rifaximin “Chaser” in Recurrent CDI • 8 women each with 4–8 prior episodes of CDI were given rifaximin (400–800 mg/d 2 wks) immediately after the last course of vancomycin before recurrence of symptoms: 1/8 (12%) had a further recurrence. • Update by Dr. Johnson to a total of 13 patients treated with vancomycin followed by rifaximin is that 3/13 (23%) had subsequent recurrence. • 2 of 3 recovered recurrence isolates had MICs >256 mg/L to rifaximin. Johnson S et al. CID 2007;44:846-8, Anaerobe 2009;15:290-291
Rifaximin Resistance 9 of 14 (64%) rifamycin resistant isolates were of the BI/NAP1/027 type. Rifaximin resistance correlated with rifampin resistance by agar dilution and E-test Acquisition of resistance in strain CF following rifaximin treatment was associated with a single amino acid change in rpoB at H502Y. MIC 0.0039 µg/ml MIC >256 µg/ml O’Connor et al AAC 2008; 52:2813-7
Current Status of Probiotics and IVIG • There is no conclusive evidence to support CDI prophylaxis or therapy with probiotics. • Data for use of IVIG for either multiple recurrences of CDI or fulminant CDI remain inconclusive as there have been no prospective randomized trials for either indication. Dendukuri et al CMAJ 2005;173:167-70, Miller M Anaerobe 2009;15:281-4 Gerding & Johnson, submitted.