Download
1 / 43
480 likes | 717 Vues
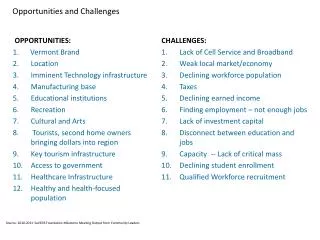
Opportunities and Challenges of SUS. Roger Dewhurst Director of Operations, Information Centre for health and social care. What are “secondary” uses ?. A considerable amount of information is collected during the provision of care and supporting services

E N D
Opportunities and Challenges of SUS Roger Dewhurst Director of Operations, Information Centre for health and social care
What are “secondary” uses ? • A considerable amount of information is collected during the provision of care and supporting services • The primary purpose of this information is to support and improve individual patient care • However, this information is of value for many other purposes to support healthcare and providing appropriate steps are taken to meet confidentiality obligations, this information can legitimately be used to support these other purposes. These are called “secondary uses” [amended from CRDB Secondary Uses Report, August 2007]
Identifiable Pseudonymised or Anonymised Primary and SecondaryUses Business Operations Commissioning Analysis / Service Planning Operational Direct Care Strategic / Policy / Research Examples of characteristics of requirements • Individual records • Selected “lists” of records • Immediate access • Dynamic, up to date • Workflow, rules based alerts • Frequent abstracts • Focus on classes • of persons • Time series • Short time intervals • Prospective indicators • Focus on classes • of persons • Actual compared with • expected • (inputs, outcomes) • Ongoing • Indicators • Focus on classes or cohorts • of persons • Disease, Service and • population • based • Forecasting • Periodic
Objectives of SUS • Improve access to data to support the business requirements of the NHS and its stakeholders • Provide a range of software tools and functionality which enable users to analyse report and present this data • Be the single, authoritative and comprehensive source of high quality data to • enable linkage of data across all care settings • ensure the consistent derivation of data items and construction of indicators for analysis • improve the timeliness of data for analysis purposes • Provide a secure environment which enables patient confidentiality to be maintained according to national standards
What is SUS? • A single repository of person and care event level data relating to the NHS care of patients. • Data is submitted by all organisations providing NHS care • At present SUS receives data submissions (CDS) relating to: • Accident and emergency attendances • Outpatient attendances • Admitted patient care, including maternity care • Elective admission waiting lists • Mental health care “spells” • In 2007/8 SUS will also receive data from Choose and Book and the Patient Demographics Service, as well as new CDS relating to future appointments and diagnostic events • In future SUS may receive data relating to patients’ prescriptions and may have the capability of managing data relating to the primary and social care provided to patients and service users.
What is SUS? • SUS comprises: • A common and consistent information governance model • Access control • Use of pseudonyms to replace identifiers • Design (e.g. small number suppression etc.) • A core data warehouse and data marts • Consistent metadata and reference data • Associated applications utilising data from the core warehouse • Consistent analysis and reporting tools
Current SUS Components Security and confidentiality ensured by consistent access control and design NHS Comparators Landing Staging Web based application for Practices, PCTs, SHAs Universal Data Warehouse HES A Core Warehouse and Data Marts Data submitted by all providers of NHS “acute” and Mental Health Care HES reports and extracts PBR NHS CDS Extract Other Extract Clinical Audit Consistent metadata – business and technical Extracts for Non NHS organisations Extracts and Reports to all PCTs, Trusts, SHAs
What has been achieved? • First release in 2005, with core NWCS and PbR functionality but suffered from: • Poor performance • Difficulties with interchange catch-up • SUS “get well” programme of work • PbR 06/07 delivered in March 2006 • Decommissioning of NWCS required focus on Release 2006-B-1 in November 2006 • Further defects and issues some of which still need to be addressed • BUT … SUS is still dependent on NHS organisations for timeliness and quality of data
SUS Releases in 2007/8 • Release 1 for PBR 07/08 and data for PBC comparators (April 2007) – completed • Release 2 giving non-functional upgrade to Oracle 10g and uplift for more users – completed • Release 3L providing “landing” capability for cds v6, plus loads from PDS and Choose and Book (CAB)– December 07 • Release 3R providing processing and reporting for 18 weeks and further reporting for CAB and PDS, includes changes necessary for PbR 2008/9 – April 08
SUS Releases in 2007/8 • NHS Comparator releases (April and September) – completed • Early reporting of comparative referral to treatment waiting times and elective pathways – early January • Additional comparators and presentation of practice level data, with particular emphasis on support for practice based commissioning resource allocation and budget setting – end January • Extended range of comparators and refresh underlying data, including dispensed prescriptions (Detailed content to be agreed with DH and NHS users) – end March • Data quality dashboard - initial release December, subsequent releases during January –March, sponsored by the DH 18 week team
Opportunities • A single secure data management environment provides an opportunity to reduce “transaction costs” of implementing systems reforms through: • Enabling access to data • Deriving essential data items consistently and once • Undertaking standard processing
Opportunities • A single secure data management environment provides the ability to construct consistent comparators and indicators
A framework for developing indicators for an “NHS Scorecard” Quality Indicators Service Outputs Indicators relate to / cover: “Population” Needs Identified Population Needs Expressed demand for services “Population” Outcomes Service Activities Service Inputs Demand Indicators Health Status Indicators Effectiveness Indicators Indicators are constructed for: Efficiency / Productivity Indicators Populations or groups of patients Providers Services Commissioners
Data to construct indicators Quality Indicators • Operational data • person and activity specific • (e.g. CDS) • aggregated returns. • dispensed prescriptions • Population and target group • based surveys, including • Patient experience • Temporal analysis of outputs • subsequent revisions etc. Service Outputs “Population” Needs Identified Population Needs Expressed demand for services “Population” Outcomes Service Activities Service Inputs Demand Indicators Health Status Indicators Effectiveness Indicators Local and national “disease / disability Registers” (within GP Clinical Systems (QOF) etc., Cancer Registries) provide identified prevalence Efficiency / Productivity Indicators • Population based surveys, which • are required to • establish unidentified need • calibrate local measures of • identified need • Operational data • included or implied in activity • specific (CDS) • Employee data from ESR • Financial returns and accounts • Operational data • person and activity specific • (e.g. CDS) • aggregated returns.
How SUS might support indicator construction and presentation Quality Indicators • SUS warehouse includes • operational data on outputs and their value /cost • NHS Comparators • includes indicators of quality of service, based on linkage of outputs • SUS functionality in 2008/9 • could enable “longitudinal” • association of operational data • with survey population (s) Service Outputs “Population” Needs Identified Population Needs Expressed demand for services “Population” Outcomes Service Activities Service Inputs Demand Indicators Health Status Indicators Effectiveness Indicators • NHS Comparators • uses data on identified need from QOF in • construction of indicators • Future releases will compare identified • prevalence and predicted prevalence • from population survey information Efficiency / Productivity Indicators • Original SUS vision and NASP • contract scope includes • workforce data as well as (costed) activity data • could enable construction and • comparative analysis of efficiency • or productivity indicators • SUS 2008/9 releases • provide for capture and management of prescriptions issued • SUS warehouse includes • operational data on activities and expressed demand (e.g. CDS) • NHS Comparators • enables comparisons of demand indicators and quality indicators covering variation in • access to services • SUS functionality in 2008/9 to support • Cohort Management and PDS based linkage • could enable “longitudinal” association of • operational data with survey population (s) • PDS copy may allow construction of prevalence models as well as linkage
Challenges • Ensuring that the data currently submitted to and managed within SUS is: • Comprehensive • Timely (for different uses) • Consistent with agreed standards • Accurate
Immediate Data Quality Challenges • Improving the coverage of data • Missing data • Creation of duplicate records • Improving the content of individual records • Linkage of data • Correct access to and exchange of data • Correct financial payments • Correct comparators and indicators • Reduction in the unnecessary use of identifiable data
Addressing Data Quality Challenges • IC / CfH • Ensure improved functionality in SUS • Tracker • eDQRS • Data Deletions • Publish guidance and provide support • Publish data on quality and enable comparison • DH / SHAs • Performance manage organisations to improve quality • Regulators and Auditors • Audit and review data quality • Commissioners • Secure improvements through contract processes • Care Providers • Implement quality assurance programmes
Immediate local implementation challenges • Achieving the migration to XML submissions • Improving the timeliness of data submissions • Migrating from the use of bulk protocols for data submission
Context for moretimely submissions • Timely data to support achievement of 18 weeks target for referral to treatment • Linkage of activity into elective care pathways • Multiple providers within pathways • Prospective analysis and reporting • Ensure at least monthly submission of comprehensively coded CDS to support PbR • Mandate of SUS as authoritative source of information for payments
Context • Operating framework for 2008/9 • Submission of finished activity within 5 working days of activity “finish” date • X % by July 2008 • Y % by January 2009 • Submission of completed (fully coded) data within 22 days of the activity “finish” date from April 2008
Benefits • Reduces processing time and complexity • 90% of records replaced in bulk updates are unchanged • Quicker access to data • Improved linkage • Reduces interchange rejection rates • Reduces the risks of duplicate records
Challenges • Supporting NHS analysis requirements, while ensuring the security and confidentiality of identifiable data: • Meeting the Government’s commitment to minimise the use of such data for non-direct care purposes
Information Governance • Governance - develop & manage consistent, cohesive policies, processes and decision rights • NHS IG - ways & means of handling patient information in legal, secure, efficient & effective manner • Balance - sharing information and privacy • Impact - Encourage & enable improvements inquality and handling of information
Context • Common law of confidence • Data Protection Act • DH Policy Guidance Confidentiality • Care Record Guarantee • This guarantee is our commitment that we will use records about you in ways that respect your rights and promote your health and wellbeing • Care Record Development Board • Secondary Uses Working Group
CRDB Principles forSecondary Uses 1.Default - use of data not linked back to individuals • Unidentifiable data (aggregate or anonymise) • Where linkage required - pseudonymise • If patient identifiable, informed consent if feasible 2. Patient right - to determine no identifiable information about them should be used for secondary purposes (legal exceptions) • Participation in research - approach through GP or relevant clinician
CRDB Principles forSecondary Uses 3.Identifiable data is required, if consent not feasible, then formal justification for access is required • Section 60 H&SC Act 2001 (now S251 Health Consolidation Act 2006) • PIAG Approval may be granted if: • Benefit to patients • Not feasible to gain consent or use anonymous data 4. All users of data for secondary care purposes should be subject to enforceable standards regarding confidentiality and security of data
Use of patient identifiable data • Originating clinician – e.g. GP in their practice • Relevant clinician – e.g. GP in their practice • Section 60/251 approval from PIAG • Role allows – e.g. 18 weeks manager • Patient’s consent – e.g. research • Legal basis – e.g. court orders
Implications • De facto use of pseudonymisation for patient record level data for secondary use • For PCTs - data for commissioning - pseudonymise • For Providers - analysis of performance,etc - pseudonymise • For practices - for practice based commissioning - pseudonymise • Where primary use of secondary use data, then patient identifiable data is OK, depending on user’s rights
CRG Requirements • CRG enables patients to use • Dissent to Store • Dissent to Share • Sealed and Locked Envelopes • Sealed Envelopes • For secondary uses • Dissent to store & Sealed and Locked Envelopes - no data available • Dissent to share & Sealed Envelopes - data available but not attributable to patient
Current SUS Data Flows HES HES Reports and Extracts Reports and extracts for Commissioners and Providers CDS Pseudon Stage Land PbR SHA and national PbR extracts Commissioning Dataset Submissions CDS Activity Warehouse Extracts for non NHS Organisations With PIAG approval
Future SUS Data Flows Other Data Flows e.g. Clinical Audits Reports, extracts and analyses from other systems and HES SUS IG Components Other Systems e.g. Audit Pseudon Cohort Linkage Geo - Derive HES SUS PDS Copy PDS Tracing 18 week CDS Reports and extracts for SHAs, commissioners and Providers Stage Land Commissioning Dataset Submissions PbR CAB Pseudonymised extracts for non-NHS organisations CDS and CAB Activity Warehouse
Challenges • Ensuring that the data submitted to and available within SUS in the future meets requirements • “redefining the information model” • “filling the gaps”