Download
1 / 121
1.22k likes | 1.95k Vues
Male Reproductive System. Chapter 48 10/20/08. Anatomy of the Male Reproductive System. The male reproductive system consists of the scrotum, testes, epididymis, vas deferens, seminal vesicles, prostate gland, ejaculatory duct, internal urethra, and penis. Scrotum .

E N D
Male Reproductive System Chapter 48 10/20/08
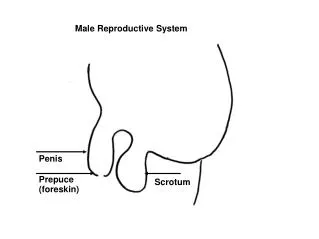
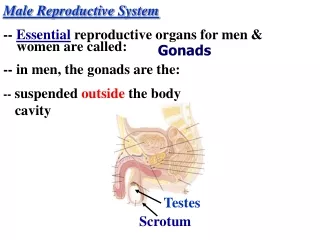
Anatomy of the Male Reproductive System • The male reproductive system consists of the scrotum, testes, epididymis, vas deferens, seminal vesicles, prostate gland, ejaculatory duct, internal urethra, and penis
Scrotum A thin sac that encloses each of the two testicles in separate compartments.The scrotum contracts into thick folds during fear, anger, arousal, or cold,drawing the testes close to the body for protection and insulation.
The two testes (Testicles) are the male reproductive organs. • They are composed of numerous tubules that produce spermatozoa and sex hormones. • The testicles develop in the embryo at about the 7th week of gestation. • They descend into the scrotum during the last 2 months of gestation. • At around 10 to 13 years of age, during puberty, the increased production of testosterone results in the production of sperm and the development of body hair, muscle mass, and other secondary sex characteristics.
Epididymis • Newly developed sperm move from each testicle through the epididymis, acoiled tubule almost 20 feet long.
Vas Deferens • As mature sperm leave the epididymis, they enter the vas deferens, which aretubes that serve as the primary storage sites for sperm and help propel themature sperm into the urethra during ejaculation.
Seminal Vesicles • Hollow, twisted, tubular secretory glands located on the posterior side of the bladder. • They produce a mucoid fluid that constitutes about 60% of the volume of semen and provides nutrients and hormones important for motility and successful fertilization.
Prostate Gland • A walnut-sized fibromuscular gland that surrounds the neck of the urinarybladder and the first inch of the internal urethra. • It produces a thin, milky, alkaline liquid that enhances the motility and fertility of the sperm and contracts to propel semen into the urethra during ejaculation
Cowper's Glands • Pea-sized structures, located just below the prostate, that secret a clearmucous into the urethra. The secretion provides lubrication during sexualarousal.
Urethra • The urethra extends from the bladder to the urinary meatus at the end of thepenis. Although the urethra serves to empty urine from the bladder andprovide outflow for semen during ejaculation, urine and semen are never in the urethra at the same time.
Penis • The external penis in its flaccid state is a soft, round cylinder ending in an acorn-shaped tip known as the glans. • The glans has a sensitive ridge at its base called the corona that gives rise to a hood or foreskin. • About one half of the penis extends within the body toward the anus and attaches to the pelvis. • Two corpora cavernosa lie on the upper side of the penis. • These erectile chambers provide a huge surface area for the inflow of blood and blood storage, which results in expansion of the penis during sexual arousal,called an erection.
Spermatogenesis • Sperm are produced in the testes from about age 13 throughout the remainderof life. • Testosterone is believed to set in motion the division of germinal cells into spermatocytes, which develop into sperm. • The process may take 75 days.
The function of the scrotum is essential for spermatogenesis. • An increase in testicular temperature may cause degeneration of some of the cells and may contribute to sterility.
Cryptorchidism, or failure of the testicles to descend from the abdomen into the cooler scrotum, may result in sterility. • If fetal testes do not secrete enough testosterone to cause the testicles to descend, surgical intervention is unlikely to be successful. • The tubular epithelium of the testes thatremain in the warm abdomen degenerates completely and is incapable of producing sperm.
Erection • For the penis to become erect, it must have a high pressure supply of arterial blood, a means of relaxing the smooth muscle tissue of the cavernosal arterioles, and a functioning blood storage mechanism to keep the blood in the penis long enough for sexual function. • The blood pressure in the flaccid corpus cavernosa is about 6 to 8 mm Hg--very low when compared with the 120/90 mm Hg blood pressure in the arm or cavernosal artery.
During sexual arousal, parasympathetic nerves release neurotransmitters that cause the cavernosal arteriole walls to relax. • This increases the blood volume of the penis to 8 to 10 times the flaccid volume. • The elastic limitations severely decrease the drainage of blood from the chamber sinuses and maintain erection. • After stimulation ceases or ejaculation occurs,sympathetic nerves release constricting neurotransmitters that narrow the arteriole walls and decrease the inflow of blood. • The penis returns to flaccid state.
Emission and Ejaculation • Emission is the result of sympathetic stimulation leaving the spinal cord at L1 and L2. • Physical stimulation of external and internal sex organs initiatescontractions of the vas derferens and prostatic capsule. • The contractions move sperm to the ejaculatory ducts and expel them into the internal urethra. • The filling of the urethra excites nerves in the sacral region of the spinal cord to initiate rhythmic muscular contractions of the internal genital organs, pelvis, and body trunk and results in ejaculation of semen.
Age-Related Changes • Assessment of the male reproductive system should include information onchanges in the patient's health, sexual function, and sexual relationships,as well as patient's knowledge level and ability for self-care. Establishinga comfortable relationship with the patient is most successful when usingopen-ended questions.
Health History • If the symptoms are acute, detailed information about the onset anddevelopment of the problem and about activities related to the symptomsshould be documented. • Medications should be noted because many drugs, including antihypertensives, can impair sexual function. • Past medical history, family history and a complete review of systems with a focus on male reproductive system as well as functional assessment will be performed
Physical Examination • The physical examination is usually done by a physician or nursepractitioner. • The patient is instructed to empty the bladder before the examination and to collect a urine specimen if needed. • The skin of the external organs and perineum should be warm, dry, and free of lesions. edema, and odor.
Scrotum • The left testicle hangs lower than the right. • Both should be oval in shape, smooth, firm, and without masses or tenderness. • It is important, especially in the young patient, to note that there are two testes. • If abnormalities are discovered, they can be further investigated by shining a light through thescrotum in a darkened room (transillumination). • Hydrocele, a mass filled with serous fluid, glows red in the light. If the mass is solid(e.g., a hematocele or tumor), no light passes through it, making it appear as a dark shadow.
Laboratory & Diagnostic TestsPage 1083 • Semen Analysis • Endocrinologic Studies • Urinalysis • Blood Studies • CT • Ultrasound • Table 48-1~Laboratory Tests • Chart ~The Male Reproductive System~ Page 1086
Laboratory Studies • Analysis of the semen may be done to assess male fertility or to documentsterilization after a vasectomy. • The patient is instructed to abstain fromsexual activity for 2 to 3 days and then collect a semen specimen in a cleancontainer. • The specimen should be kept at room temperature protected form heat or cold and brought to the lab within one hour • Gross evaluation of semen for volume, thickness, color and pH as well as sperm count , motility , shape and ability to penetrate cervical mucous will be examined. • Discourage patients from prolonged abstinence because it may result in diminished quality and motility of the sperm.
Endocrinologic Studies • The endocrine system secretes hormones directly into the blood that regulate metabolism, growth, stress response and reproduction. • Testosterone is secreted by Leydig cells in the testes. • Below-normal levels of testosterone may be the result of hypothalamic or pituitary dysfunction orseminiferous tubule destruction. • The causes of increased levels of testosterone in the adult male are testicular tumor, adrenal tumor, adrenal dysfunction, and some drugs (anticonvulsants, barbiturates). • Testosterone levels fall with age, beginning around age 30.
Endocrinologic Studies • Follicle-stimulating hormone (FSH) is secreted by the anterior pituitary gland and causes stimulation of Stertoli cells in the testes to complete theformation and maturation of sperm. • Luteinizing hormone (LH) is secreted bythe anterior pituitary gland and causes stimulation of Leydig cells in the testes to produce testosterone. • Prolactin, another hormone secreted by theanterior pituitary gland, has a potentiating effect on testosterone production.
Tumor Markers • Tumor markers are substances found in the serum of cancer patients. • Prostate-specific antigen (PSA) is used as a screening tool to detect prostate cancer. • Annual PSA screening is recommended for all men after age 50 (high risk age 40). • There is no special preparation for this test.
General Laboratory Studies • Blood studies may include a CBC in forming a diagnosis when anemia or bone metastases are suspected. • Alkaline phosphate and serum calcium levels also may be measured because they increase with metastasis to the bone. • The acid phosphate level also may be increased with prostate cancer and with bone metastasis.
Radiologic Imaging Studies • A CT may be used in assessing metastatic testicular and prostate tumors. • Ultra sound may be used to examine scrotal masses or define prostatic lesions. • Examination of the prostate is done via the rectum.
Radionuclide imaging may be done to assess testicular abnormalities such as torsion, tumors, abscesses, epididymitis or hydrocels. • Radioactive substances are injected intravenously or given orally. • After a waiting period to allow for distribution of the substance throughout the body, scans are done to locate organs and tissues that have increased concentrations of the isotopes due to abnormal tissue metabolism.
Infections and Inflammatory Conditions • The most common inflammatory conditions are prostatitis and epididymitis. • Orchitisis rare, but important because it can cause sterility.
Prostatitis • An inflammation of the prostate gland. • There are four categories of prostatitis: acute bacterial prostatitis, chronic bacterial prostatitis, chronic prostatitis/chronic pelvic pain syndrome, and asymptomaticinflammatory prostatitis. • Inflammation caused by bacterial infection can beacute or chronic. • The patient who has prostate pain but no evidence ofinfection is said to have chronic prostatitis/chronic pelvin pain syndrome. • When no pathogens can be detected, the condition is classified as asymptomatic inflammatory prostatitis.
A 4 week course of antibiotics usually is prescribed for acute bacterialprostatitis, and up to 16 weeks of therapy for chronic bacterial prostatitis (Bactrium/Cipro) • Chronic prostatitis/chronic pelvic pain syndrome may be treated with a shortcourse of antibiotics, but it often is ineffective. • Anti-inflammatory drugsor opiod analgesics may be used.
The patient is advised to increase fluid intake and to rest. • Stool softners may be prescribed to prevent constipation, which is especially painful withprostatitis. • Urethral catherization is contraindicated with urethralinflammation, but suprapubic catherization may be necessary if the patient has difficulty voiding.
Asymptomatic inflammatory prostatitis may be treated with a single daily doseof an alpha-adrenergic blocker to improve voiding by relaxing the bladderneck and prostate. • Symptoms are managed with analgesics, anti-inflammatory agents, and sitz baths. • Prostate massage and ejaculation may be helpful with some types of prostatitis because they drain excess prostatic secretions.
Epididymitis • An inflammation of the epididymis. Signs and symptoms are painful scrotaledema, nausea, vomiting, chills, and fever. • Epididymitisis treated with bedrest, ice packs, sitz baths, analgesics, antibiotics, anti-inflammatory drugs, and scrotal support. • A bridge made of tape and gauze or a rolled towel can be placed across the patient's thighs while in bed to elevate the scrotum and reduce pain.
Orchitis • An inflammation of one or both of the testes. It may be related to trauma orto infections such as mumps, pneumonia, or tuberculosis. • Signs and symptoms include fever, tenderness and swelling of the affected testicle, and scrotal redness. The inflammation can lead to reduced fertility or sterility.
BPH (Hyperplasia)Page 1088 • Benign prostatic hypertrophy is enlargement of the prostate gland. • It is a common age-related change, the exact cause is unknown. • Diagnosis is based on rectal examination, laboratory and radiographic studies, endoscopy, ultrasound, catheterization for residual urine and sometimes urodynamic testing.
Signs and Symptoms • Signs and symptoms of BPH are described as obstructive or irritative. • Obstructive symptoms include decreasing size and force of the urinary stream,urine retention, and post-void dribbling. • Irritative symptoms include urgency, frequency, dysuria, nocturia, hematuria, and sometimes urge incontinence. • Factors that may trigger retention are alcohol, infections, delayed voiding, bed rest, opiods, antihistamines, and chilling.
Consider the alternative--Saw Palmetto effectively relieves urinary symptomsassociated with BPH without reducing the size of the prostate. Also, itreduces serum levels of PSA, which could give a false-negative result inpatients with prostate cancer.
Medical Treatment • 5-alpha reductase inhibitors suppress prostatic tissue growth by decreasingtestosterone levels > Finasteride (Proscar) • Alpha-adrenergic blocking agents are used to relax smooth muscle in thebladder neck and prostate, thereby reducing obstruction to urinary flow >tamsulosin (Flomax) terazosin (Hytrin)
Surgical/Invasive Treatments • In general, invasive procedures involve surgical removal of all or part ofthe prostate (prostatectomy) or ablation (destruction) of prostate tissue.
Types of Prostatectomy • The most widely used surgical procedure is the transurethral resection of the prostate (TURP), in which obstructing portions of the gland are cut away through a resectoscope inserted into the urethra. • There is no external incision. Atriple-lumen urinary catheter commonly is used to maintain continuous irrigation and bladder drainage
A suprapubic prostatectomy is performed through the bladder by way of a lowabdominal incision. • This may be selected when the prostate is very large or when there are also bladder abnormalities that require surgical correction. • Some patients develop incontinence or erectile dysfunction.