Download
1 / 6
60 likes | 89 Vues
ROCK Study Group Case of the Month. Benton Heyworth, MD Assistant Professor, Department of Orthopaedic Surgery Boston Children ’ s Hospital. Patient Profile. Patient (EC) 18-year old male High school basketball player, aspirations of collegiate play

E N D
ROCK Study Group Case of the Month Benton Heyworth, MD Assistant Professor, Department of Orthopaedic Surgery Boston Children’s Hospital
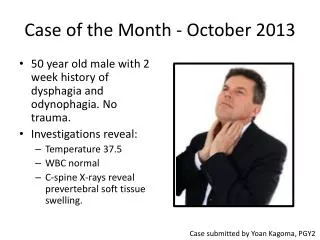
Patient Profile • Patient (EC) • 18-year old male • High school basketball player, aspirations of collegiate play • No past medical, surgical, or relevant family history • Presented to sport medicine clinic on 5/16/17 • HPC • April 2017, fell on flexed right knee • Persistent lateral knee pain, swelling, “soreness with prolonged walking”, feeling of loose body “moving around inside knee” • PE • Neutral bilateral lower extremity alignment in the coronal plane • Full strength and ROM in bilateral hips, knees, and ankles • Intact sensation bilaterally • Right knee: lateral joint pain, trace effusion, mild pain with hyperflexion; negative patellar grind, no severe crepitus, ligaments intact
Imaging • XR (5/7/2017) • Trochlear lucency, no clear evidence of loose bodies (osteochondral fragments likely w/ demineralized bone) • MRI (5/7/2017) • 22 x 11 x 8 mm crater in the midportion of the lateral trochlear ridge • Full thickness cartilage and subchondral bone loss with at least 3 small osteochondral fragments seen either within the lesion or outside • Normal patellar cartilage
Surgical Options Assessment • 18yo Mbasketball player w/ large, oval-shaped crater/osteochondraldefect in the lateral trochlear ridge • No evidence of single/intact/sufficiently-sized fragment (18 x 8 mm) to attempt fixation Plan • Options: • OATS • If two snowman type bone plugs can be fit • MACI • OC Allograft • RLB + Microfx • Other • De Novo, Biocartilage, Cartiform, etc • First surgery 5/18/17: • Removal of loose bodies • Assessment of viability of OATS procedure • to be scheduled for future date if pursued • Harvest of cartilage if MACI pursued
1 Initial Surgery 5/18/2017 • Diagnostic arthroscopy • Positive findings • Trochlea: large chondral defect with subchondral bone involvement, 22 x 11 mm crater (Image 1) • Intercondylar notch: large loose body (chondral/osteochondra,l 18 x 11 x 8 mm) (Image 2) • OATS assessment • Sizing of lesion • 12 mm incision, lateral to the patella • 10 mm OATS sizer was inserted • Able to fit into the bottom of the defect (1 mm wider than would allow for optimal Press-Fit OATS technique) (Image 3) • Moreover it was felt to measure 22 mm and appeared longer than the double stacked two plug snowman type technique would allow • Therefore it was felt that a cultured chondrocyte cartilage resurfacing technique would be optimal for this lesion with use of bone graft and sandwich technique • MACI Harvest • Site- lateral aspect of the intercondylar notch (in the area of an ACL notchplasty, NOT involving the weight bearing cartilage) • Specimen- cartilage with a small amount of attached subchondral bone • Biopsy sent to Vericel for cultured chondrocyte preparation 2 3
MACI Procedure 2 8/24/2017 Arthrotomy • A lateral parapatellar arthrotomy incision measuring 6 cm was made between the prior superolateral portal and the inferolateral portal from his prior procedure and extended up to the vastus lateralis distally and above the level of the meniscus in the capsular level taking care to protect the lateral edge of the patellar tendon and leave a small cuff of tissue for repair just lateral to the patella Lesion preparation • Of note at this time the two loose bodies were seen and removed • 11 blade and a ring curet providing a strong stable edge of a tall white cartilage on all sides • The sclerotic bone at the base of the lesion was burred with a high-speed bur until punctate cancellus bleeding was seen • The lesion was measured with standard technique and attention was turned towards the bone grafting. Bone graft harvest • Site- proximal tibia • The superolateral aspect inside the joint but above the level of articular cartilage was identified and a rent through the synovium made down to the level of the periosteum which was elevated to expose 1 x 1 cm area of lateral cortex • The 4.5 drill bit was used and spun to be able to access bone graft with a curved curet • An adequate amount of bone graft was obtained and then the periosteum and overlying synovium closed with figure-of-eight stitches to achieve hemostasis • A tamp was used to impact the bone graft and then fibrin glue using the Tisseel syringe was impressed onto the top of the bone graft and then held in place with a finger, achieving good stability of the bone graft material MACI cell implantation • Sandwich technique • A second layer of glue was placed and the MACI which had been cut using the template previously measured was put into place and laid flat. Good stability of the layer was seen and the tourniquet was let down to ensure hemostasis. With pressure of a saline-soaked neuro patties for several minutes, good hemostasis was seen and a second layer of glue placed though somewhat thinner. • The second layer of the MACI membrane was put this time with the cells facing down such that cells were on the inside of both layers of "sandwich." The edges of the MACI membrane were then affixed using fibrin glue. Care was taken to ensure that no portion of the MACI membrane extruded superficial to the level of the articular cartilage and was well contained within the defect. However the bone graft had been impacted and glued essentially up to the level of the adjacent normal subchondral bone. The knee was taken through range of motion and the layer was found to be stable and untouched.