Download
1 / 37
380 likes | 641 Vues
Learn about the history, classification, pathogenesis, and prevention of poliovirus infection, including details on Enteroviruses, Poliovirus, and clinical manifestations.

E N D
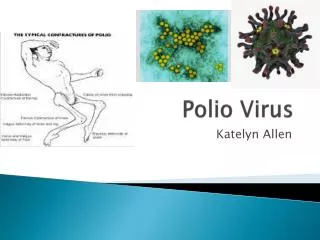
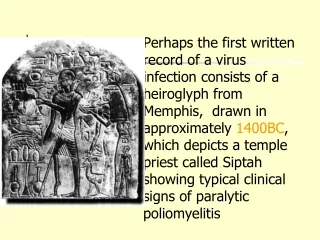
Perhaps the first written record of a virus infection consists of a heiroglyph from Memphis, drawn in approximately 1400BC, which depicts a temple priest called Siptah showing typical clinical signs of paralytic poliomyelitis
20 – 30 nm • Icosahedral capsid • Non-enveloped • Positive sense RNA • Can be cultivated in human or moneky cell cultures
Classification - Picarnoviridae • Enterovirus • Parechovirus • Hepatovirus • Aphthovirus • Cardiovirus
Enteroviruses • Enteroviruses are a genus of the picornavirus family which replicate mainly in the gut. • Single stranded naked RNA virus with icosahedral symmetry • Unlike rhinoviruses, they are stable in acid pH • Capsid has 60 copies each of 4 proteins, VP1, VP2, VP3 and VP4 arranged with icosahedral symmetry around a positive sense genome.
At least 71 serotypes are known: divided into 5 groups • Polioviruses 1-3 • Coxsackie A viruses 1-24 • Coxsackie B viruses 1-6 • Echoviruses 1-33 • Enteroviruses (more recently, new enteroviruses subtype have been allocated sequential numbers (68-71)
Poliovirus was first identified in 1909 by inoculation of specimens into monkeys. • The virus was first grown in cell culture in 1949 which became the basis for vaccines
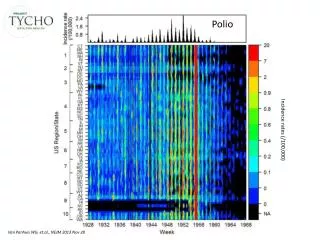
Poliovirus • 3 serotypes of poliovirus (1, 2, and3) but no common antigen. • Have identical physical properties but only share 36-52% nucleotide homology. • Humans are the only susceptible hosts. • Polioviruses are distributed globally. Before the availability of immunization, almost 100% of the population in developing countries before the age of 5. • The availability of immunization and the poliovirus eradication campaign has eradicated poliovirus in most regions of the world except in the Indian Subcontinent and Africa. • Poliovirus is on course of being eradicated worldwide by the end of 2000 or 2001.
Pathogenesis • The incubation period - 7 - 14 days. • virus multiplies in the oropharyngeal and intestinal mucosa. • The lymphatic system, in particular the tonsils and the Peyer's patches of the ileum are invaded and the virus enters the blood resulting in a transient viraemia. • In a minority of cases,the virus may involve the CNS following dissemination.
The central nervous system may be invaded by way of the circulating blood. Large amounts of anti-body are necessary to prevent passage of the virus along nerve fiber. • Poliovirus can spread along axons of peripheral nerves to the central nervous system, along the fibers of the lower motor neurons to the spinal cord or the brain. • Virus invades certain types of nerve cell, and may da-mage or completely destroy these cells for its intracell-ular multiplication.
Clinical Manifestations There are 3 possible outcomes of infection: • Subclinical infection (90 - 95%) – in-apparent subclinical infection account for the vast majority of poliovirus infections. • Abortive infection (4 - 8%) - a minor influenza-like illness occurs, recovery occurs within a few days and the diagnosis can only be made by the laboratory. The minor illness may be accompanied by aseptic meningitis
Major illness (1 - 2%) - the major illness may present 2 - 3 days following the minor illness or without any preceding minor illness. • Signs of aseptic meningitis are common. • Involvement of the anterior horn cells lead to flaccid paralysis. Involvement of the medulla may lead to respiratory paralysis and death.
Laboratory Diagnosis Microscopy – EM /IEM for stool specimen Virus Isolation • poliovirus can be readily isolated from throat swabs, faeces, and rectal swabs. It is rarely isolated from the CSF • Cell culture - Primary monkey kidney cells, HeLa and Hep-2 • Cytopathic effect - Swelling, lysis, cellular disorganization Serology • Very rarely used for diagnosis since cell culture is efficient. Occasionally used for immune status screening for immunocompromised individuals.
Prevention Intramuscular Poliovirus Vaccine (IPV) SALK • consists of formalin inactivated virus of all 3 poliovirus serotypes. • Produces serum antibodies only: does not induce local immunity and thus will not prevent local infection of the gut. • However, it will prevent paralytic poliomyelitis since viraemia is essential for the pathogenesis of the disease. • Oral Poliovirus Vaccine (OPV) SABIN • Consists of live attenuated virus of all 3 serotypes. • Produces local immunity through the induction of an IgA response as well as systemic immunity. • Rarely causes paralytic poliomyelitis, around 1 in 3 million doses.
Prevention • Most countries use OPV because of its ability to induce local immunity and also it is much cheaper to produce than IPV. • The normal response rate to OPV is close to 100%. • OPV is used for the WHO poliovirus eradication campaign. • Poliovirus has been eradicated from most regions of the world except the Indian subcontinent and sub-Saharan Africa.
Coxsackieviruses • Group A viruses produce a diffuse myositis with acute inflammation and necrosis of fibers of voluntary muscles. • Group B viruses produce focal areas of degeneration in the brain, necrosis in the skeletal muscles, and inflammatory changes in the dorsal fat pads, the pancreas and occasionally the myocardium. • Each of the 23 group A and 6 group B coxsackieviruses have a type specific antigen. • In addition, all from group B and one from group A (A9) share a group Ag. Cross-reactivities have also been demonstrated between several group A viruses but no common group antigen has been found.
COXSACKIE A • Aseptic meningitis • Herpangia – type 2,4,6,8 &10 • Hand-foot-and mouth disease – Type 5 & 16 COXSACKIE B • Epidemic myalgia • Myocarditis & pericarditis • Asceptic meningitis • Juvenile diabetes • Neonatal infections
Exanthems -Rubelliform rashes • - EV leading cause in summer & fall. All types of rash
Hand-foot-and-mouth disease • Hand-foot-and-mouth disease: mostly coxackie A • fever, malaise, sore throat, vesicles on bucal mucosa, tongue, hands, feet, buttocks • highly infectious • resolution – 1w
Herpangina • Herpangina – usually coxackie A • acute onset, fever, sore throat, dysphagia • lesions – posterior pharynx • can persist w’s • no gingivitis
Echoviruses • The first echoviruses were accidentally discovered in human faeces, unassociated with human disease during epidemiological studies of polioviruses. The viruses were named echoviruses (enteric, cytopathic, human, orphan viruses). • These viruses were produced CPE in cell cultures, but did not induce detectable pathological lesions in suckling mice. • Altogether, There are 32 echoviruses (types 1-34; echovirus 10 and 28 were found to be other viruses and thus the numbers are unused) • There is no group echovirus Ag but heterotypic cross-reactions occur between a few pairs.
New Enteroviruses • Newly identified picornaviruses that are not polioviruses are no longer classified separated into the species coxsackie and echovirus because of the ambiguities presented by overlapping host range variations. • 4 new enteroviruses have been identified (68 - 72). Enterovirus 70 is the causative agent epidemics of acute haemorrhagic conjunctivitis that swept through Africa, Asia, India and Europe from 1969 to 1974. The virus is occasionally neurovirulent. • Enterovirus 71 appears to be highly pathogenic and has been associated with epidemics of a variety of acute diseases, including aseptic meningitis, encephalitis, paralytic poliomyelitis-like disease and hand-foot-mouth disease. • Enterovirus 72 was originally assigned to hepatitis A virus, but it had now been assigned to a new family called heptoviruses.
Disease Associations (1) • Paralytic Disease - most commonly associated with polioviruses but other enteroviruses may also be responsible, notably enterovirus 71 • Meningitis - caused by all groups of enteroviruses, most commonly seen in children under 5 years of age. • Encephalitis - focal or generalized encephalitis may accompany meningitis. Most patients recover completely with no neurological deficit. • Undifferentiated febrile illness - may be seen with all groups of enteroviruses. • Hand foot mouth disease - usually caused by group A coxsackieviruses although group B coxsackieviruses and other enteroviruses have been caused outbreaks. • Herpangina - caused by group A coxsackieviruses. • Epidemic Pleurodynia (Bornholm disease) - normally caused by group B coxsackieviruses.
Disease Associations (2) • Myocarditis - group B coxsackieviruses are the major cause of myocarditis, although it may be caused by other enteroviruses. It may present in neonates as part of neonatal infection and is often fatal. In adults, the disease is rarely fatal. • Respiratory Infections - several enteroviruses are associated with the common cold. • Rubelliform rashes- a rash disease resembling rubella may be seen with several coxsackie A, B, and echoviruses. • Neonatal Infection - some coxsackie B viruses and echoviruses may cause infection in newborn infants. The virus is usually transmitted perinatally during the birth process and symptoms vary from a mild febrile illness to a severe fulminating multisystem disease and death. • Conjunctivitis - associated with several types of enteroviruses, notably Coxsackie A24 and Enterovirus 70 (haemorrhagic conjunctivitis) • Pancreatitis/Diabetes - associated with Coxsackie B virus infection. The extent of the role of the virus in diabetes is unknown.
Laboratory Diagnosis • Virus Isolation • Mainstay of diagnosis of enterovirus infection • Coxsackie B and Echoviruses can be readily grown in cell culture from throat swabs, faeces, and rectal swabs. They can also be isolated from the CSF • Coxsackie A viruses cannot be easily isolated in cell culture. They can be isolated readily in suckling mice but this is not offered by most diagnostic laboratories because of practical considerations. Molecular techniques may provide a better alternative. • Serology • Very rarely used for diagnosis since cell culture is efficient. • Neutralization tests or EIAs are used but are very cumbersome and thus not offered by most diagnostic laboratories
Cytopathic Effect (Virology Laboratory, New-Yale Haven Hospital)
Management and Prevention • There is no specific antiviral therapy available against enteroviruses other than polio. • Some authorities use IVIG in the treatment of neonatal infections or severe infections in immunocompromised individuals. However, the efficacy is uncertain. • HNIG have been to prevent outbreaks of neonatal infection with good results. • There is no vaccine available mainly because of the multiplicity of serotypes. There is little interest in developing a vaccine except against enterovirus 71 and coxsackie B viruses.
Rhinoviruses • Rhinoviruses primarily infect the nose and the throat. Rhinoviruses resemble other picornaviruses in size and structure. • They replicate optimally at 33oC (the lower temperature of the nose) and they are acid labile, inactivated below pH 6. • This explains why rhinoviruses are restricted to nose and the throat. Man is the only natural host and there are more than 100 serotypes of rhinoviruses (117 to date).
Pathogenesis: • Rhinoviruses (rhino – nose, the organ primarily affected) cause common cold. They are transmitted by droplet infection. They remain strictly localized to the nose and throat and do not spread. After an incubation period of 2 – 4 days, patient develops watery discharge with nasal obstruction, sneezing, cough, headache, sore throat, and malaise. The uncomplicated illness subsides in a week.
HEPATOVIRUS • Although it was first classified as enterovirus 72, the nucleotide and amino acid sequences of HAV are sufficiently distinct to assign it to a new picornavirus genus, Hepatovirus. Only one serotype is known. • Transmission of the virus occurs by faeco-oral route via contaminated food or water. Virus replicates in the gut and reaches the liver by hematogenous route following a brief viraemic period. HAV causes infectious hepatitis, and the clinical illness is characterized by fever, gastrointestinal symptoms such as nausea and vomiting, and jaundice