Download
1 / 25
250 likes | 540 Vues
Advanced Practice of Pharmacy Experience: Journal Club Mai Nguyen Mercer University COPHS Doctor of Pharmacy Candidate 2012 Preceptor: Dr. Ali Rahimi October 20, 2011. General Overview. Background.

E N D
Advanced Practice of Pharmacy Experience: Journal ClubMai NguyenMercer University COPHSDoctor of Pharmacy Candidate 2012Preceptor: Dr. Ali Rahimi October 20, 2011
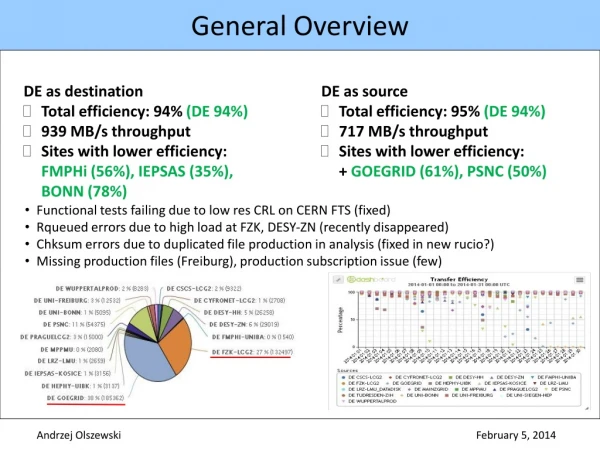
Background • Atrial fibrillation is associated with an increase in the risk of ischemic stroke by a factor of 4 to 5 and accounts for up to 15% of strokes in persons of all ages and 30% in persons over the age of 80.1 • Current guidelines for preventing stroke in patients with atrial fibrillation recommend using warfarin, a vitamin K antagonist, with a target INR of 2-3, as the standard care of therapy. • However, warfarin has many food and drug interactions, and requires frequent monitoring and dose adjustments.
Background • Rivaroxaban (Xarelto®):3 • First oral, selective inhibitor of Factor Xa approved by the FDA on July 1, 2011. • FDA indicated for prophylaxis of deep vein thrombosis (DVT) which may lead to pulmonary embolism (PE) in patients undergoing knee or hip replacement surgery. • Convenient once daily, oral dosing • No need for routine monitoring of INR or other coagulation parameters.
Objective • To compare once daily oral rivaroxaban with dose-adjusted warfarin for the prevention of stroke and systemic embolism in patients with nonvalvular atrial fibrillation who were at moderate to high risk for stroke. • Primary hypothesis: rivaroxaban is noninferior to warfarin for the prevention of stroke or systemic embolism.
Study Population • Inclusion Criteria: • Men or women aged ≥ 18 years with nonvalvular atrial fibrillation (ECG evidence), who were at moderate-to-high risk for stroke. • Elevated risk factors: history of stroke, transient ischemic attack, or systemic embolism OR • At least 2 of the following risk factors: heart failure or left ventricular ejection fraction of ≤ 35%, hypertension, age ≥ 75 years, or DM • Female subjects must be postmenopausal, surgically sterile, or abstinent. • If sexually active, must use effective method of birth control before entry and throughout the study. • Must have a negative pregnancy test at screening.
Study Population • Baseline Demographics: • Median age was 73 years • 39.7% women; 60.3% male • 90.5% of patients had hypertension • 54.8% of patients had previous stroke or systemic embolism • 62.4% of patients had previous use of warfarin • Baseline characteristics did not differ significantly between the two treatment groups.
Interventions • 14,264 patients were randomly assigned to receive: • Fixed-dose rivaroxaban 20 mg daily or15 mg daily in patients with CrCl 30-49 mL/min AND placebo (n = 7,131) • Dose-adjusted warfarin (target INR 2.0-3.0) AND placebo (n = 7,133)
Interventions • Patients were seen at weeks 1, 2, and 4, then monthly for duration of study to measure INR, primary endpoint events, TIA, MI, medical/surgical procedures, adverse events and vital stats • Median duration of treatment: 590 days • Median follow-up period: 707 days
Statistical Analysis • Primary Analysis: • Performed in the per-protocol population • Included all patients who received at least one dose of a study drug, did not have major protocol violation, and were followed for events while receiving drug or within 2 days after discontinuation. • Power of 95% • 363 events needed; study used 405 events • One-sided significance level of 0.025
Statistical Analysis • If noninferiority was achieved in the primary analysis, • Primary Superiority Analysis: • Performed in the as-treated safety population • Included patients who received at least one dose of a study drug and were followed for events, regardless of adherence to the protocol, while they were receiving the assigned study drug or within 2 days after discontinuation. • Two-sided significance level of 0.05 • Key secondary endpoints were also tested for superiority in the as-treated safety population.
Statistical Analysis • Testing for noninferiority and superiority was also performed in the intention-to-treat population • Included all patients who underwent randomization and were followed for events during treatment or after premature discontinuation • Hazard ratios, confidence intervals, and P values were calculated using Cox proportional-hazards models • Warfarin group: • Rosendaal method - calculate overall time that INR values fell within therapeutic range
Statistical Analysis • Hazard Ratio (AKA Relative Risk or Risk Ratio): • The ratio of risk of an outcome event occurring in the experimental group compared to the risk of the same outcome event occurring in the control group. • HR < 1.0 indicates the therapy decreasedthe risk of developing the adverse outcome • HR = 1.0 indicates no difference between treatments • HR > 1.0 indicates the therapy increased the risk of developing the adverse outcome
Results – Calculations • NNT (primary endpoint – stroke and systemic embolism): • ARR = 241/7,004 – 188/6,958 = 0.0074 • NNT = 1/0.0074 = 135 • NNH (safety endpoint – major and nonmajor bleeding): • ARI = 1,475/7,111 – 1,449/7,125 = 0.004 • NNH = 1/0.004 = 250
Author’s Conclusion • In patients with atrial fibrillation, rivaroxaban was noninferior to warfarin for the prevention of stroke or systemic embolism. • There was no significant difference in the risk of major bleeding between groups, although intracranial and fatal bleeding occurred less frequently in the rivaroxaban group.
Evaluations limitations Strengths Randomized, double-blind, multi-center study with a large sample size Treatment groups appeared similar at baseline Included almost 40% females Duke Clinical Research Institute coordinated the trial, managed database, and performed primary analyses independently of the sponsors. • In warfarin group, INR values were within therapeutic range only 55% of the time. • Switching from per-protocol population to as-treated safety population to achieve superiority. • The primary endpoint of stroke was a composite of ischemic and hemorrhagic strokes. • No inclusion of data for increased GI bleeding
Conclusion and Application • Rivaroxaban is a potential alternative to warfarin, especially for patients with compliance issues. • Things to consider: • Cost • No Antidote • Monitoring for coagulation parameters needed • How to bridge patients when switching from warfarin to rivaroxaban? • Long-term effects?
References • Patel MR, et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. New England Journal of Medicine. 2011; 365:883-891. • Supplement to: Patel MR, et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. New England Journal of Medicine. 2011; 365:883-891. DOI: 10.1056/NEJMoa1009638. • Xarelto® (rivaroxaban) Product Package Insert. 2011; July. Janssen Pharmaceuticals, Inc. Titusville, NJ.