About the Midterm
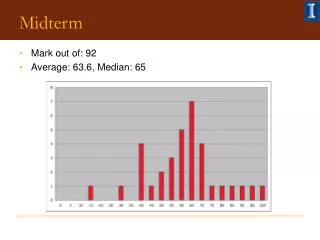
About the Midterm. Grades are posted Class average = 89 Overall GREAT JOB! Thanks for feedback. OBgyn Week 7. Normal Pregnancy. Conception. Traditionally, involves a fertile woman and a fertile man.

About the Midterm
E N D
Presentation Transcript
About the Midterm • Grades are posted • Class average = 89 • Overall GREAT JOB! • Thanks for feedback
OBgyn Week 7 Normal Pregnancy
Conception • Traditionally, involves a fertile woman and a fertile man. (These days can involve egg donors, sperm donors, surrogates, fertility hormones, artificial implantation, and other techniques which will not be covered in this lecture) • Possible during fertile window of woman’s cycle (around ovulation) • Sperm must travel through cervix, uterus, fallopian tubes to reach and fertilize egg
Conception • Sperm undergo enzymatic reactions (while traveling through cervical mucus and fallopian tubes) to help penetrate the protective layers around the ovum • Sperm chemically attracted to ovum • Progesterone • Follicular fluid from ovum
Conception • Fertilization occurs in Fallopian tube, zygote (fertilized egg) continues to divide as it travels to uterus and implants • Takes 3-4 days for embryo to reach uterus • Implantation generally occurs ~3-4 days after embryo enters the uterus
Fertile Days of Cycle Factors to consider: • Ovulation occurs ~day 14 (anytime of day) • Ovum can survive up to 24 hours after ovulation • Sperm can survive in the vagina up to 48 hours after ejaculation • So fertile window is ~days 11-16 of cycle (if trying to conceive, these are best days; expand to ~days 8-19 if trying NOT to conceive) • strict day correlation depends on cycle regularity • remember - follicular phase can vary in length
Fertility Symptoms • Charting of menses • Helps determine fertile days, esp if regular cycles • Cervical mucus • Will be thicker, stretchy when most fertile • Cervical position and feel • Cervix softens, moves further from introitus when fertile • Basal body temp • Increases just after ovulation • Hormone levels • LH surges prior to ovulation (must draw blood to test) • Salivary crystallization • At-home test kits available
Multiples • Most commonly twins or triplets • May arise from: • Release and fertilization of multiple ova (fraternal twins) • Division of zygote into two embryos (identical twins) Division during stage when cells are totipotent • Combination of these • Identical triplets or quadruplets also possible • High risk of pre-term delivery, low birth weight
Early Pregnancy Sx All of these are due to hormone level changes: • Nausea / vomiting (esp in AM) • Commonly lasts until ~week 12-15, when placenta takes over roll of hormone production from corpus luteum • Swollen / tender breasts • Mood changes / irritability • Fatigue • Leucorrhea: white, thicker vaginal discharge • Lack of menstrual period • Will have been pregnant ~2 weeks by this point • May have light spotting lasting ~1 day (more may be sign of spontaneous abortion or of ectopic pregnancy)
Abnormal Sx Symptoms of ectopic pregnancy or spontaneous abortion may include: Cramps Severe abdominal pain Bleeding Spotting > 1 days Fainting or Dizziness
Pregnancy Diagnosis • Urine b-HCG - accurate at time of missed period (home test kits available OTC) • Serum b-HCG - quantitative tests most sensitive • Ultrasound (abdominal) • 5-6 weeks can see gestational sac • 8 weeks can see heart beat to assess viability Vaginal Ultrasound can determine heart beat, gestational sac at 5 weeks
Later Signs of Pregnancy • Softening and bluing of cervix • Enlargement of uterus (may be palpated by 15 wks) • Fetal heart tones (Doppler or fetascope) • 120-160bpm, so easy to tell apart from mother’s • May be detected as early as 10 wks • Lack of FHT by 12-14 weeks is concerning, may be due to: • Wrong date determination • Non-viable fetus • Posterior position of fetus • Thick abdominal wall • Retroflexed uterus
Later Signs of Pregnancy • Quickening: first fetal mvmt felt by the mother • Primiparous: 18-20 weeks • Multiparous: 16-19 weeks • Braxton Hicks contractions: localized uterine contractions that may start at 20 weeks; very irregular and variable • At 20 weeks, ballotment: moveable baby
Length of Pregnancy • Estimated Due Date = 40 weeks (280 days) after first day of last menstrual period • Naegle’s rule: subtract 3 months from LMP, add 7 days, add 1 year • Add 266 days from exact day of conception • 85% of women deliver around EDD; 10% early, 5% late • “Normal” can vary from 37-42 weeks • LMP used to estimate gestational age • And remember, fertilization usually occurs ~2 weeks after first day of LMP • Conception age refers to date of probable conception • ~2 weeks less than gestational age
Establishing EDD • Difficulties with establishment of Due Date • Irregular or abnormal menses • Miscarriage • Lactation (annovulatory for 6-12 months) • Gynecological problems (e.g. polycystic ovaries) • Other interfering factors • Low dose OCPs • Early or late ovulation • Poor recording of menstrual history
Establishing EDD • Importance of establishing correct EDD • Determine pre or post maturity • Important if home birth (safe to deliver weeks 37-42; if premature or postdate, need to refer to hospital) • Determine IUGR (Intrauterine growth retardation) • Determine multiple pregnancy or abnormal levels of amniotic fluid • Determine paternity • Gestational age important in considering TAB, amniocentesis, alpha fetal protein
Maternal Changes • Weight gain • Loosening of joints • Hormonal changes • Increase in blood volume • Enlargement of uterus, crowding of abdominal and pelvic organs • Enlargement of breasts
Weight Gain • Normal weight gain ~30 lbs if healthy weight at start of pregnancy ~9 of these lbs are weight of fetus, placenta, amniotic fluid, uterine hypertrophy, increased blood volume, breast enlargement, maternal intra/extracellular volume • Variables to weight gain: • Age, parity, income, maternal education, etc. • Large weight gain associated with LGA (large for gestational age) babies • Contributes to maternal obesity, gestational diabetes, increased risk for CV dz and diabetes later in life • Low weight gain associated with SGA babies • Greater risk for preterm labor
Maternal Weight Gain • National Academy of Science recommendations according to BMI • 28-40# for underweight women • 5# in first trimester; >1# week thereafter • 15-35# for women at normal weight • 2-4# in first trimester; 1# week thereafter • 15-25# for overweight women • 2# in first trimester; <1# week thereafter
Physiologic Changes • Cervical changes: effacement and dilation • Thick clot of mucus in cervical os: mucous plug • Cervix softens and becomes cyanotic (increased vascularity) • Change in consistency in cervical mucus • Uterine changes: • Displaces intestines laterally and superiorly • Increases tension on on broad and round ligaments • Uterus also undergoes irregular contractions • Unpredictable, nonrhythmic, aka Braxton-Hicks • Vaginal changes: • Softening of tissues • Increased cervical mucus • Decreased pH (3.5 to 6) (antibacterial function?)
Phys Changes • Ovaries • Ovarian function ceases, maturation of new follicles suspended • Corpus luteum produces progesterone (until ~week 12, when placenta takes over this function) • Corpus luteum also secretes relaxin hormone • Changes in breasts: • Increased tenderness in first weeks • Increase in size • Nipples become enlarged and more deeply pigmented • Colostrum secreted pre or post-natally
Phys Changes • Musculoskeletal changes • Softening of ligaments (esp. sacro-illiac and pubic symphisis) due to relaxin hormone • Lumbar lordosis • Loosening of all joints • Often noticed as increase of foot length / shoe size • Skin changes: • chloasma (“mask” of pregnancy) • linea nigra on abdomen • striae • increased hair growth, increased perspiration
Phys Changes - CV • Cardiovascular changes • Increased cardiac outflow by 30-40% • Increase in blood volume by >35% • Increase in body mass (enlarged uterus) • Facilitates blood flow/ gas exchange to placenta • Protects mother against excessive blood loss during labor • Greater increase in plasma than erythrocytes • Benign ejection systolic heart murmurs • Increased pulse rate 10-15bpm (How would you expect her pulse to feel?) • Edema of pregnancy • Increased capillary pressure and permeability • Fetal pressure in pelvis decreases venous return of lower half of body
More Physiologic Changes • Increase in cellular respiration for fetus/placenta and mom • Shortness of breath dt restriction on diaphragm • Kidneys about 1 cm larger during pregnancy • Increase in dental caries • Decreased secretion of HCL and pepsin • Decreased gastric emptying and intestinal motility • Increased metabolic rate by 20%
Endocrine Changes • Increased thyroid function (free, active thyroid hormone T3 remains the same) • Incrased prolactin, cortisol, aldosterone • Decreased GH, FSH, LH • Difficulty balancing blood glucose • Glucose as energy source favored by fetus • Estrogen increases 1000x (ovaries and adrenals) • Progesterone increases 10x
Estrogen Effects • Influences growth and fxn of uterus, breasts, labia • Increases pliability of CT, joint relaxation • Increases adipose tissue (fat stores) • Increases skin pigmentation • Increases Na+ and volume retention • Stimulates 3rd trimester prostaglandin production • Associated with mood swings • Increases insulin production/ secretion as well as tissue sensitivity to insulin • Increases uterine receptivity to progesterone and oxytocin
Progesterone Effects • Produced by corpus luteum, then by placenta • Increases the blood supply of endometrium • Suppresses maternal immunological response to fetus • Inhibits contraction of uterus • Relaxes smooth muscle (bladder tone, slows GI motility) • Radically decreases at labor onset
More Endocrine Changes • Prolactin • Produced by maternal and fetal pituitary glands, uterus • Sustains milk production and regulates milk composition • Prostaglandins • Produced by mother, fetus, placenta • Soften cervix, prime maternal body for labor • Oxytocin • Produced by hypothalamus, released by pituitary • Stimulates uterine contractions, milk let down/ ejection • Distension of cervix and vagina stimulates release of oxytocin and prostaglandins during labor
Endocrine Changes - HCG • bHCG (beta human chorionic gonadotrophin) • Secreted by fetus starting day 6-8 • Prevents degeneration of corpus luteum so that E and P continue to be secreted • Maximum levels at 7-16 weeks • At 8-12 weeks, promotes testosterone synthesis and secretion for male sexual differentiation • Used in diagnosis for quantitative pregnancy tests/ ectopic pregnancy
Endocrine Changes - HPL • HPL (human placental lactogen) • aka HCS (Human Chorionic Somatomammotropin) • Produced by placenta • Decreases maternal insulin sensitivity • Elevates maternal blood glucose levels with decreased maternal glucose usage = more available for fetus • Elevated during hypogycemia to mobilize free fatty acids for energy for maternal metabolism • Increases lipolysis • Glucose preferentially used as fuel by fetus, maternal energy increasingly comes from fat stores • Decreases hunger sensation and diverts maternal CHO metabolism to fat metabolism in 3rd trimester • Plateaus in 3rd trimester
Trimesters • Pregnancy divided into trimesters, each ~3 months (13-14 weeks) • 1st : weeks 0-13 • 2nd : weeks 14-28 • 3rd : weeks 29-40
Week-by-Week Developments • First Trimester (embryonic development) *Highly sensitive to teratogens during this stage* • Weeks 1 and 2: remember, this is preconception: mother’s body prepares for ovulation, fertilization • Wk 3: fertilization occurs, cell division begins • Wk 4: CNS begins to develop, angiogenesis, primitive cardiovascular system • Wk 5: neurogenesis, brain activity, heart beat HCG levels detectable via home test kits • Wk 6: embryo size of a bean, face developing • Wk 7-8: Eyes, hair, all essential organs, movement • Wk 8: Embryonic stage over, fetal stage begins
First trimester continued • Wk 9-12: dvpmt of fetal muscle, cartilage, genitals, Fetal Heart Tones detectable • Wk 13: fetus is about the size of a peach • Common maternal symptoms: • Morning sickness, breast tenderness/swelling, fatigue, weight gain, constipation, heartburn, food cravings, frequent urination • Recommendations: • Focus on good nutrition: nutrient-dense and fiber-rich foods, avoid refined carbs, eat small, frequent meals • Ginger, acupuncture to relieve nausea • Gentle exercise to aid circulation, bowel mvmts, fatigue • Kegel exercises now to help prevent incontinence later
Fetal development2nd trimester (wk 14-28) Further organ development and function Fetus swallows fluid, urinates, sleeps and wakes • Week 16: toes, fingers, eyelashes • Wk 17: fetus can hear outside noises; mom may start to be visibly pregnant, may feel “quickening” • Wk 20: gender identification possible with ultrasound • Wk 21: mom SOB, fetus presses against diaphragm • Wk 24: Check baby’s position; if born at this time, there is a chance of survival of infant Lack of lung dvpmt, low body weight are greatest risk factors • Wk 25: all organs formed, now mainly growth; risk for pre-eclampsia begins
2nd trimester • Common maternal symptoms: • Striae, linea nigra, hemorrhoids and other varicosities, increased allergen sensitivity, swollen feet/ankles, shortness of breath • Increased incidence of dental caries (cavities) • Recommendations: • Continue to focus on good nutrition • Rest, nap, put feet up periodically • Good oral hygiene especially important
Fetal development3rd trimester (wk 29-40+) Fetal weight gain ~1 ounce/day Brain develops rapidly: Maternal nutrition - omega 3s • Wk 33: fetus moves downward, head down • Wk 34: testes descend (in male fetus) • Wk 37: lung surfactant produced • Wk 38-40: ready for delivery! • Wk 41-42: still within normal, low-risk range U.S. averages for infants at term birth: Female wt: 7 lbs, male wt: 7.5 lbs, length: 20”
Placenta • New organ (!) develops for pregnancy only • Develops from embryonic cells (outer layer of blastocyst) • Allows gas exchange (oxygen, CO2) without mixing of maternal and fetal circulation • Also permeable to vitamins, glucose, free fatty acids and electrolytes, and antibodies
Placental Circulation • Mother’s circulation connects through uterine wall • Fetal circ from placenta via umbilical cord • Placental circulation reverse of convention • Arteries carry deoxygenated blood • Veins carry oxygenated blood
Placenta in Multiples • Depends on: • Dizygotic twins v. monozygotic twins • Time at which cleavage of monozygote occurred • A= dizygotic twins (two sperm fertilized two eggs) • B= monozygotic twins, cleavage of zygote 4-8d post fertilization • C= monozygotic twins, cleavage of zygote 8-12d post fert.
Nutrition - general • Early fetal development • Folate: needed for proper brain and CNS development - must have good levels at very start of pregnancy to prevent defects • B12: also needed for proper fetal CNS dvpmt • Vitamin A: overdoses can cause defects, so important not to megadose during pregnancy • Prenatal vitamins • Maintenance of pregnancy • Extra calories (~100-300 more/day) • Quality fats (including omega 3s), oils, and protein • Nutrient-dense, fiber-rich foods • Avoid refined carbs and “empty” calories!
Nutrition • Do not restrict salt during pregnancy! • Electrolytes needed to balance increased blood volume • Low sodium diet can lead to elevated BP (drop in blood volume makes kidneys react as if hemorrhage occurred and release renin, which constricts blood vessels) • No weight-loss diets during pregnancy! • If pt overweight, focus on healthy food choices • Protein needs increase (60-100g/day) • Increased risk for Pregnancy-induced hypertension with malnutrition, low protein, low calories and low salt • Can monitor protein status by checking serum albumin
Nutrition - minerals • Iron • 30mg/day (60-90mg/d if mom anemic) • Better taken with vitamin C, away from tannins • Calcium • 600-1200mg/ day supplemental to dietary intake • Increased PTH stimulates calcium release from bones • No net bone loss during pregnancy, but bone loss can occur during lactation with inadequate calcium intake • Deficiency: muscle spasm, bleeding gums, headache • Zinc • 15-30mg/day; >30mg may be teratogenic • Important for protein synthesis • Deficiency associated with: infertility, chronic SAB, PIH, dysfunctional labor, infections
Nutrition - folate • Folic acid * Start taking before pregnancy* • 800-1000mcg/day • Needed for DNA synthesis, protein metabolism, neurological development • Deficiency assoc with neural tube defects (spina bifida) • Deficiency common in vegan diets, smoking, OCP use • Should always supplement with Vitamin B12, as it can mask symptoms of B12 deficiency
Nutrition - vitamins • B vitamins • 25% women in US are deficient in B vitamins • 50mg/day B6 • Helps with nausea/ vomiting • B12 deficiency results in CNS defects in baby • Esp. important for vegans to supplement B12 • Vitamin C • 500-1000mg/d • Megadoses (10g) may cause miscarriage in early weeks • May also interfere with pregnancy test results • Decreased incidence of SIDS if taken during pregnancy and continued while breast feeding
Nutrition - vitamins • Vitamin A • Use beta-carotene in pregnancy as high doses of vit A may be teratogenic (>10,000IU) • Be aware of patients using vitamin A as skin treatment (acne, wrinkles) • Vitamin D • Recent research: deficiencies increase risk for C-section • Sunshine is best source • Supplement doses determined by serum vitamin D levels
Nutrition - prenatal vitamins • Take before and throughout pregnancy • Most necessary vitamins and minerals are included in prenatal formulas • May need extra iron if anemic • Need omega 3 fatty acids (not included) • And, of course, still need a good diet