Download
1 / 37
400 likes | 550 Vues
Explore the liver's vital functions in metabolism, detoxification, and homeostasis of nutrients. Learn about its role in carbohydrate, lipid, and protein metabolism, as well as biotransformations.

E N D
Biochemistry of liver Alice Skoumalová
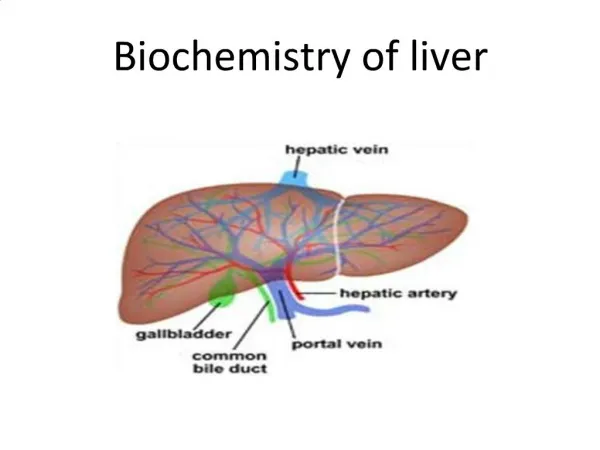
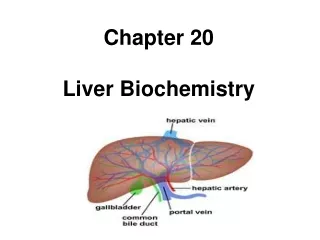
The liver-introduction • importance in intermediary metabolism and in the detoxification and elimination of toxic substances • one of the largest organs in the human body • it constitutes only 2-3% of the body mass, it accounts for 20-30% of the total oxygen consumption
Diagram of a hepatocyte There are approximately 300 billion cells in the liver (80% of them are hepatocytes) The hepatocytes are central to the intermediary metabolism of the body
Functions of the liver • The uptake of nutrients delivered from the digestive tract via the portal vein • The synthesis, storage, interconversion, and degradation of metabolites (metabolism) • The regulated supply of energy-rich intermediates and building blocks for biosynthetic reactions • The detoxification of harmful compounds by biotransformation • The excretion of substances with the bile, as well as the synthesis and degradation of many blood plasma constituens • Fighting infections (Kuppfer cells-macrophages)
Liver metabolismThe primary function is the maintenance of sufficient plasma levels of the metabolites (homeostasis) • Carbohydrate metabolism • Lipid metabolism • Amino acid and protein metabolism • Biotransformations
Liver metabolismThe primary function is the maintenance of sufficient plasma levels of the metabolites (homeostasis) • Carbohydrate metabolism: 1. The liver takes up glucose and other monosaccharides from the blood plasma -These sugars are then converted to glucose 6-phosphate and other intermediates of glycolysis (subsequently, they are either stored as the reserve carbohydrate glycogen or degraded) -Another large part is converted into fatty acids -Only a small fraction is used for the generation of ATP 2. The liver secretes glucose when there is a major decline in the blood glucose level -This glucose is derived from the glycogen store -If the glycogen store is already exhausted, glucose can also be synthesized by gluconeogenesis from lactate, glycerol, or the backbones of amino acids • Lipid metabolism • Amino acid and protein metabolism • Biotransformations
Liver metabolismThe primary function is the maintenance of sufficient plasma levels of the metabolites (homeostasis) • Carbohydrate metabolism • Lipid metabolism: 1. The liver synthesizes fatty acids from acetate units -The fatty acids formed are then used for the synthesis of fats and phospholipids (these are subsequently released into the blood as complexes with proteins-lipoproteins) 2. The liver can take up fatty acids from the plasma -The conversion of fatty acids into ketone bodies, which are also excreted 3. The liver also uses acetate units to synthesize cholesterol -It is then transported to other organs as a constituent of plasma lipoproteins 4. Excess cholesterol is converted into bile acids or excreted with the bile • Amino acid and protein metabolism • Biotransformations
Liver metabolismThe primary function is the maintenance of sufficient plasma levels of the metabolites (homeostasis) • Carbohydrate metabolism • Lipid metabolism • Amino acid and protein metabolism: 1. The liver controls the amino acid level of the plasma -It breaks down excess amino acids -The nitrogen thus released is converted to urea and transported to the kidneys -The carbon skeletons of the amino acids enter intermediary metabolism, where they are consumed either in the synthesis of glucose or in the production of energy 2. The liver is the site of the synthesis and degradation of most proteins and peptides in the blood plasma • Biotransformations
Liver metabolismThe primary function is the maintenance of sufficient plasma levels of the metabolites (homeostasis) • Carbohydrate metabolism • Lipid metabolism • Amino acid and protein metabolism • Biotransformations 1. Steroid hormones and degradation products of the blood pigment hemoglobin are taken up by the liver -They are inactivated and converted into highly polar metabolites 2. Drugs, ethanol, and other foreign substances (xenobiotics) are metabolized by similar reactions -Preparation for excretion
The role of the liver in nutrition The tissues are dependent on a constant supply of energy-rich metabolites to provide energy and as precursors for the synthesis of complex macromolecules • The liver: 1. It compensates the variation of the level of these fuels in the diet (buffering organ) 2. It supplies with metabolites (storage organ) • Biochemistry of nutrition: 1. Well-fed (= absorptive state) -The energy requirements of the tissues are predominantly met by glucose 2. Starvation (= postresorptive state) - The energy requirements of the tissues are met mainly by fatty acids, amino acids, and ketone bodies (exceptions: nerve tissue and erythrocytes) The transition between these two states depends on the levels of energy-rich metabolites in the blood plasma (it is brought about by the joint action of hormones and signals from the nervous system)
The role of the liver in carbohydrate metabolism • The concentration of glucose in the blood is maintained constant (at 4-6 mM) -this is achieved by the precise regulation of glucose- forming and glucose-utilizing pathways • In the liver, glucose is derived from: 1. Glycogenolysis 2. Gluconeogenesis 3. Fructose and galactose metabolism 4. Cori cycle (from lactate) 5. Alanine cycle (from alanine)
Liver glycogen • Glycogen serves as a carbohydrate reserve, from which glucose can be released • The human body can store up to 450 g of glycogen (a third in the liver) • Liver glycogen serves in the maintenance of the blood glucose level, it declines to zero in periods of starvation that last more than one day
Liver gluconeogenesis • The glycogen reserves are already depleted after one day • The blood glucose level begins to fall • An increase of gluconeogenesis
Liver gluconeogenesis • Gluconeogenesis occurs predominantly in the liver (90%) • Precursors: 1. Amino acids derived from the muscles (prolonged fasting results in a massive degradation of muscle protein) 2. Lactate formed in erythrocytes and in muscles 3. Glycerol produced from the degradation of fats • Cortisol, glucagon, epinephrine: promote gluconeogenesis • Insulin: inhibits gluconeogenesis
Cori and alanine cycles Alanine cycle: Degradation of proteins: -the amino groups are transferred to pyruvate, giving rise to alanine Alanine is transported to the liver: -the carbon skeleton is converted into glucose, -nitrogen is converted into urea Cori cycle: Lactate (anaerobic glycolysis) -transported to the liver -converted back into glucose via gluconeogenesis Glucose- is sent back to its site of utilization
The role of the liver in lipid metabolism The liver is the most important site for the formation of fatty acids, fats, ketone bodies, and cholesterol • Absorptive state: -The liver converts glucose via acetyl-CoA into fatty acids -The liver can also retrieve fatty acids from lipids supplied with chylomicrons from the intestine -The fatty acids are converted into neutral fats and phospholipids, VLDL are formed (transport of fatty acids to other tissues) • Postresorptive state: -The adipose tissue releases fatty acids -Fatty acids are taken up by the liver and oxidatively degraded to acetyl-CoA -Acetyl-CoA is converted to ketone bodies
Biosynthesis of ketone bodies • Acetyl-CoA (ß-oxidation): -can be oxidized by the citric acid cycle -when the acetyl-CoA production exceeds the energy requirements of the hepatocytes (starvation, diabetes mellitus) they form ketone bodies (supply other tissues with energy) • Ketone bodies: They are released by the liver into the blood, in which they are readily soluble (their levels are elevated during period of starvation) 3-Hydroxybutyrate and acetoacetate serve as the key metabolites in energy production (after 1-2 weeks of starvation, the nerve tissue also begins to utilize ketone bodies as energy sources) Acetone is exhaled via the lungs • Ketonemia, ketosuria, ketoacidosis: when the production of ketone bodies exceeds their use outside the liver (prolonged starvation, diabetes mellitus)
Sources of cholesterol: 1. the diet, 2. de novo synthesis from acetyl-CoA (liver) • Utilization of cholesterol: 1. the synthesis of bile acids, 2. building block for cell membranes, 3. stored in the form of lipid droplets, following esterification with fatty acids, 4. formation of VLDL (supply other tissues) • The liver takes up from the blood and degrades lipoprotein complexes containing cholesterol (HDL) Cholesterol metabolism
The role of the liver in amino acid metabolism • The main site of amino acid degradation is the liver (significant quantities of ammonia are released) • Ammonia: -is toxic to cells (at higher concentrations, it is especially damaging to the nerve cells) -has to be rapidly inactivated and excreted (in human, this occurs primarily through the formation of urea) • NH3 metabolism of the liver: • Amino nitrogen, which accumulates in the tissues, is transported in the blood incorporated into glutamine (Gln) and alanine (Ala) • Gln is deaminated by glutaminase to yield NH3 and glutamate (Glu) • The amino group of alanine is transferred to 2-oxoglutarate by alanine transaminase • NH3 is released from glutamate by oxidative deamination (catalyzed by glutamate dehydrogenase) • Aspartate (Asp), the second amino group donor in the urea cycle, also arises from glutamate (catalyzed by aspartate transaminase)
Urea cycle • Urea: -It is neutral and non-toxic -It can cross membranes by diffusion (small, uncharged molecule) -It is highly soluble in water -It can be easily transported by the blood and excreted in the urine • Urea synthesis: -It occurs predominantly in the liver -Urea is formed in a cyclic series of reactions; its nitrogen atoms are derived from ammonia and aspartate, and the carbonyl carbon from hydrogen carbonate
Bile acid metabolism • Bile acids: -steroids with 24 carbons (from one to three α-hydroxyl groups and a side chain with a carboxylate group) -synthesized in the liver from cholesterol -amphipathic (have a polar and an apolar side); act as detergents -linked with an amino acid (glycine or taurine)- bile salts -primary bile acids are formed in the liver, secondary bile acids in the intestine (by dehydroxylation of the primary bile acids) • Lipid digestion: -facilitate the solubilization of dietary lipids during the process of digestion by promoting micelle formation (this action increases the effectiveness of pancreatic lipases, and promotes the absorption of lipids from the intestine)
Metabolism of bile salts (exlusively in the liver) 4. a 5. Intestinal bacteria in the colon produce enzymes that can attack and alter the bile salts 6. Most of the bile acids are reabsorbed from the intestine and, following transport to the liver, returned once again into the bile (enterohepatic circulation) 1. The biosynthesis of bile acids from cholesterol 2. The conjugation with the amino acids 3. The concentration in the gallbladder by removal of water
Biotransformations (= the detoxification and elimination; predominantly in the liver) Foreign substances: Self-substances Xenobiotics (natural origin) Steroid hormones Pharmaceuticals Bile pigments Synthetics • Transformation reactions • Either incorporate new functional groups into apolar compounds, or alter groups that are already present in the molecule • The result is an increase in the polarity and a decrease in the biological activity or toxicity of the substance The most important reactions: • Oxidative reactions: hydroxylation, epoxide formation, dealkylation, deamination • Reductive reactions • Methylation • Desulfuration Poorly soluble, biologically active, some toxic Phase I Transformation products
Biotransformations Transformation products • Conjugate formation: • These reactions couple substrates to highly polar, often negatively charged molecules • The enzymes involved are transferases • 1. Glucuronidation • 2. Esterification with sulfate • 3. Amidation with glycine and glutamate Phase II Conjugate Bile Urine
Cytochrome P450 system • Monooxygenases that contain a heme group • Enzymatic hydroxylation (phase I reactions): drugs, ethanol • Also involved in the biosynthesis of steroid hormones, bile acids, eicosanoids, and unsaturated fatty acids • Low specificity • Found in the liver, adrenal cortex • Cytochrome P450-dependent monooxygenases: reactions • The reductive cleavage of molecular oxygen (one atom is incorporated into the substrate, the other is released as water) • The reducing equivalents are derived from NADPH + H+
Cytochrome P450 system • Examples of the Cyt P450-dependent reactions: • The hydroxylation of aromatic rings (drugs, steroids) • Aliphatic methyl groups can be oxidized to hydroxyl functions • The epoxidation of aromatics yields products that are toxic (benzopyrene) • Dealkylations
Ethanol metabolism • Ethanol is rapidly taken up from the digestive tract by diffusion • The maximum blood alcohol level is reached within 60-90 minutesAlcohol is rapidly distributed throughout the organism (a large amount is taken up by muscles and the brain) • The lethal blood alcohol level is 0.3-0.4% The alcohol content of alcoholic beverages • Given as percent by volume (conversion to gram ethanol, density = 0,79 kg/l) A bottle of beer: 0,5l with 4% alcohol contains 16g of ethanol A bottle of wine: 0,7l with 12% alcohol contains 66g of ethanol
Ethanol degradation (in the liver) • Other enzymes are also involved in ethanol degradation (catalase, Cyt P450) • Alcohol dehydrogenase oxidizes ethanol to ethanal (acetaldehyde) • It is futher oxidized to acetate by aldehyde dehydrogenase • Acetate is then converted to acetyl-CoA by acetate-CoA ligase in an ATP-dependent reaction
Elevated consumption of ethanol over many years may lead to liver damage (the limit for a man is about 60g daily, and for a woman about 50g); these values are strongly dependent on body weight, health and the use of medication • The high levels of NADH and acetyl-CoA inhibit citric acid cycle activity and ketogenesis, whereas they exert a stimulatory effect on the synthesis of neutral fats and cholesterol (an increase in the storage of lipids leads to a fatty liver- it is reversible) • In chronic alcoholism- liver cell death (cirrhosis of the liver, an irreversible, progressive loss of liver function) Liver damage
Bilirubin metabolism and excretion • Bilirubin (degraded product of hemoglobin) is transported in the blood bound to albumin • The liver takes up bilirubin and conjugates it with glucuronic acid • Conjugated bilirubin is excreted via the bile ducts into the gut • It is converted to urobilinogen (most of it is oxidized to urobilin in the colon and excreted) • Some urobilinogen is absorbed from the small intestine and enters the enterohepatic circulation (most is excreted in the bile, some reached the systemic circulation and is excreted in the urine)
Hyperbilirubinemia • Elevated bilirubin levels in the blood (>10 mg/l); bilirubin may diffuse into peripheral tissues, giving them a yellow color (jaundice) • Cause: 1. Pre-hepatic: excessive formation of bilirubin by increased degradation of erythrocytes (icterus neonatus, hemolytic anemia) 2. Hepatic: insufficient processing of bilirubin as a result of liver defects (hepatitis, liver toxic damage, cirrhosis, hepatic failure) 3. Post-hepatic: by impaired excretion of gall (obstructive jaundice due to gallstones, inflammation of biliary tract) • Unconjugated bilirubin can cross the blood-brain barrier, leading to brain damage • Jaundice in neonates (increased bilirubin degradation+immaturity of the conjugation enzymes): phototerapy – isomerization of bilirubin to more soluble pigments
Biochemical assessment of liver function • Basic tests: albumin, ALT, AST, GGT, ALP, bilirubin, U-urobilinogen, U-bilirubin • Special tests: serum protein electrophoresis, prealbumin, glutamate dehydrogenase, cholinesterase, lactate dehydrogenase, oral glucose tolerance test (oGTT), P-Fe • Very special tests: ceruloplasmin, S-Cu, α1-antitrypsin, ammonia, P-bile acids, serological tests in hepatitis B, assessment of clotting factors
ALT (alanine aminotransferase): • increased when cells of the liver are inflamed or undergo cell death • rises dramatically in acute liver damage, such as viral hepatitis • AST (aspartate aminotransferase): • less specific for liver disease • raises in acute liver damage • GGT (gamma-glutamyltransferase): • produced by the bile duct (sensitive marker for cholestatic damage) • raises in alcohol toxicity • ALP (alkaline phosphatase): • associated with the biliary tract • raises in biliary tract damage and inflammation
Bilirubin -total and direct (=conjugated) • Urine urobilinogen: -insufficient function of the liver • Urine bilirubin: -when plasma direct bilirubin is elevated (obstructive and hepatocellular icterus)