Download
1 / 56
760 likes | 2.06k Vues
Biochemistry of the liver. Magdaléna Fořtová Department of Medical Chemistry and Clinical Biochemistry, 2nd Faculty of Medicine, Charles University and University Hospital Motol, Department of Nephrology, 1st Faculty of Medicine, Charles University and General University Hospital.

E N D
Biochemistry of the liver Magdaléna Fořtová Department of Medical Chemistry and Clinical Biochemistry, 2nd Faculty of Medicine, Charles University and University Hospital Motol, Department of Nephrology, 1st Faculty of Medicine, Charles University and General University Hospital
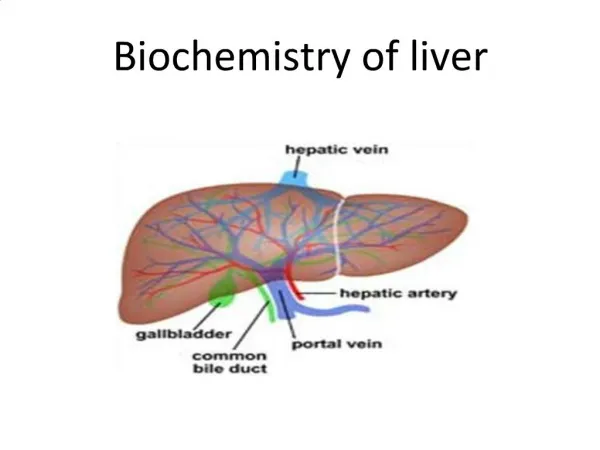
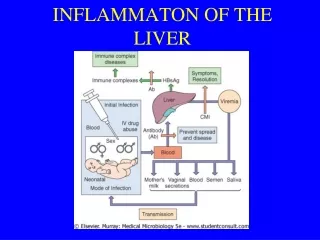
Central position in energy and intermediary metabolism • regulation of blood concentration of many metabolites • regulation of storage and production of energy • synthesis of molecules for other tissues • interconversion of nutrients • storage of some substances • formation and secretion of bile • detoxification function
Portal lobulus • Hepatic acinus Zone 1 (periportal) - is nearest to the entering vascular supply and receives the most oxygenated blood (and a lot of nutrients), making itleast sensitive to ischemic injury while making it very susceptible to viral hepatitis, hepatocytes (with more mitochondria, less ER) are specialized for oxidative liver functions such as gluconeogenesis, β-oxidation of fatty acids and cholesterol synthesis, CC, RCH, oxidative phosphorylation, urea synthesis, cholesterol synthesis, proteosynthesis (cytochrome oxidase, CC enzymes, LD, AST, ALT, GMT, ALP),occurs in phosphorus poisoning, hemochromatosis (deposition of hemosiderin) or eclampsia Zone 2 (midzonal)- rare – is seen in yellow fever Zone 3 (centrilobular, perivenous) - has the poorest oxygenation (and few nutriens), and will be most affected during a time of ischemia, cells are more important for reductive reactions,glycolysis, glycogen synthesis, ketogenesis, lipogenesis and cytochrome P-450-based drug detoxification, biotransformation of xenobiotics (sm. ER), detoxification of NH3 (synthesis of Gln) (GMD, alcohol dehydrogenase, isocitrate dehydrogenase),occurs with ischemic injury, toxic effects, carbon tetrachloride exposure or chloroform ingestion, cells have the highest concentration of CYP2E1 and thus are most sensitive to NAPQI (N-acetyl-p-benzoquinone imine) production in acetaminophen toxicity Drugs such as acetaminophen may be metabolized in zone 1 to toxic compounds that cause necrosis in zone 3
CHS, coagulations factors, plasmat.proteins DNA-ase glucuronyltransferase, detoxification GMD, mAST, CC enzymes hydrolases, kathepsin ALP, GGT, NTS ALT, cAST, LD Cytoplasm
ALT, cAST LD mAST,GMD kathepsin CHS, coag.fact. Alb., TTR ALP, GGT, NTS
DIAGNOSTIC ENZYMES Cytoplasm:ALT, cAST (30 % of total liver AST) , LD permeability dysfunction Mitochondria:mAST, GMD (glutamate dehydrogenase)necrosis Membranes of bile duct endothelium and sinusoids:ALP, GGT, 5-NTS (5´-nukleotidase)cholestasis Lysosomes:hydrolytic enzymes: proteinases (kathepsin) a β-glucuronidase(Gaucher´s disease) Rough endoplasmic reticulum:CHS (cholinesterase), coagulations factors, plasmat. proteines (albumin, transthyretin, transferrin) protein synthesis defect (decrease !)
Liver function tests Standard liver tests • Aspartate transaminase • Alanine transaminase • Alkaline phosphatase • Gamma glutamyl transpeptidase • Total, direct, and indirect bilirubin • Albumin, prealbumin, cholinesterase • INR Other tests • Other coagulation test • 5´nucleotidase • Serum glucose • Lactate dehydrogenase
Albumin • The main protein of human blood plasma, made specifically by the liver • Its main function is to regulate the colloidal osmotic (oncotic) pressure of blood. • It also serves as a carrier for molecules of low water solubility, including lipid soluble hormones (thyroxine), bile salts, unconjugated bilirubin, free fatty acids, cations (Ca2+, Na+, K+), ions and some drugs like warfarin, clofibrate, phenytoin. (Competition between drugs for albumin binding sites may cause drug interaction by increasing the free fraction of one of the drugs). • Hypoalbuminemia may be caused by chronic liver disease (such as cirrhosis), nephrotic syndrome (where it is lost through the urine), burns, protein-losing enteropathy, malabsorption, malnutrition, late pregnancy, artefact, genetic variations and malignancy. • The consequence of low albumin can be edema since the intravascular oncotic pressure becomes lower than the extravascular space. • Hyperalbuminemia is almost always caused by dehydration. • Referenge range: 3.5 to 5 g/dL, FN Motol 35 to 53 g/L
Transthyretin (TTR) • TTR was originally called prealbumin (or thyroxine-binding prealbumin) because it ran faster than albumin on electrophoresis gels. • It is better at detecting acute changes than albumin (half-life of albumin and prealbumin is 2-3 weeks and 2-4 days, respectively). • It is a serum and cerebrospinal fluid carrier of thyroxine and retinol-binding protein bound to retinol (this is how transthyretin gained its name, transports thyroxine and retinol). • Nutritional status can be assessed by measuring its concentration in the blood (other transport proteins such as albumin or transferrin could be used, but transthyretin is preferred because of its shorter half-life, although this means that its concentration more closely reflects recent dietary intake rather than overall nutritional status). • Referenge range: 15.7 to 29.6 mg/dL, FN Motol 0.18 to 0.40 g/L
RR: 67 – 190 μkat/l FN Motol Pseudocholinesterase • also known as plasma cholinesterase, butyrylcholinesterase, or acylcholine acylhydrolase, catalyzes the hydrolysis of butyrylthiocholin, benzoylcholin, sukcinylcholin and other cholin or thiocholin esters (x acetylcholinesterase, found primarily in the blood on red blood cell membranes, in neuromuscular junctions, and in neural synapses, catalyzes the hydrolysis of the neurotransmitter acetylcholine into choline and acetic acid entirely) • is produced in the liver (marker of protein synthesis) • the half-life of pseudocholinesterase is approximately 8–16 hours • Its levels may be reduced in patients with advanced liver disease. The decrease must be greater than 75 % before significant prolongation of neuromuscular blockade occurs with succinylcholine. • Genetic variants: normal activity: U (usual), reduced activity: A (atypical), F (fluoride), S (silent)…. • Acute organophosphate insecticide poisoning • An absence or mutation of the pseudocholinesterase enzyme leads to a medical condition known as pseudocholinesterase deficiency • People with pseudocholinesterase deficiency respond abnormally to succinylcholine, experiencing substantial prolongation of muscle paralysis with apnea rather than the usual 2-6 min • Dibucaine number = (1- (CHS inhibited/CHS uninhibited))*100 (normal > 80)
Alanine transaminase (ALT) • also called serum glutamic-pyruvic transaminase or alanine aminotransferase • ALT is found predominantly in the liver (in cytoplasm of parenchymal cells), with clinically negligible quantities found in the kidneys, heart, and skeletal muscle • It catalyzes the transfer of an amino group from L-alanine to α-ketoglutarate, the products of this reversible transamination reaction being pyruvate and L-glutamate L-glutamate + pyruvate ⇌ α-ketoglutarate + L-alanine ALT (and all transaminases) require the coenzyme pyridoxal phosphate, which is converted into pyridoxamine in the first phase of the reaction, when an amino acid is converted into a keto acid • It is commonly measured clinically as a part of a diagnostic evaluation of hepatocellular injury, to determine liver health. • Significantly elevated levels often suggest the existence of other medical problems such as viral hepatitis, congestive heart failure, liver damage, bile duct problems, infectious mononucleosis…. • Referenge range: 10 to 45 IU/L, FN Motol: 0,17 to 0,78 μkat/L
Aspartate transaminase (AST) • also called serum glutamic oxaloacetic transaminase or aspartate aminotransferase • a pyridoxal phosphate (PLP)-dependent transaminase enzyme • It catalyzes the reversible transfer of an α-amino group between aspartate and glutamate Aspartate (Asp) + α-ketoglutarate ↔ oxaloacetate + glutamate (Glu) • AST is found in the liver (parenchymal cells), heart, skeletal muscle, kidneys, brain, and red blood cells, and it is commonly measured clinically as a a part of diagnostic liver function tests, to determine liver health (but it is not specific to the liver, it has also been used as a cardiac marker etc.), it is raised mainly in acute liver damage • Two isoenzymes are present in humans: • cAST, the cytosolic isoenzyme derives mainly from red blood cells and heart (30 % of liver AST) • mAST, the mitochondrial isoenzyme is present predominantly in liver (70 % of liver AST) • Referenge range: 8 to 40 IU/L, FN Motol: 0,16 to 0,72 μkat/L
Transaminases Alanine aminotransferase(ALT) Aspartate aminotransferase(AST)
De Ritis Ratio • The AST/ALT ratio is sometimes useful in differentiating between causes of liver damage • In healthy people ALT > AST; when AST > ALT, pathosis is likely. Thus: • AST/ALT is normally < 1.0 and is also < 1.0 in viral hepatitis (albeit with extremely high levels of both AST and ALT). • When AST/ALT > 1.0 but < 2.0, it is likely to be associated with cirrhosis • When AST/ALT > 2.0, it is more likely to be associated with alcoholic hepatitis or hepatocellular carcinoma • However, the AST/ALT ratio is less useful in scenarios where the liver enzymes are not elevated, or where multiple conditions co-exist.
Transaminases • AST is similar to ALT in that both enzymes are associated with liver parenchymal cells (ALT occurs in cytoplasm, AST in cytoplasm, but also in mitochondria). • ALT is found predominantly in the liver, while AST is found in the liver and the other organs (cardiac and skeletal muscle etc.) ALT is a more specific indicator of liver inflammation than AST. • Many drugs may elevate ALT and AST levels, including anti-inflammatory drugs, antibiotics, cholesterol medications, some antipsychotics such as risperidone, and anticonvulsants. • AST/ALT elevations instead of ALP elevations favor liver cell necrosis as a mechanism over cholestasis. • When AST and ALT are both over 1000 IU/L, the differential can include acetaminophen (paracetamol) toxicity, shock, or fulminant liver failure. • When AST and ALT are greater than three times normal but not greater than 1000 IU/L, the differential can include alcohol toxicity, viral hepatitis, drug-induced level, liver cancer, sepsis, Wilson's disease, post-transplant rejection of liver, autoimmune hepatitis, and steatohepatitis (nonalcoholic).
Alkaline phosphatase (ALP) • is a hydrolase enzyme responsible for removing phosphate groups from many types of molecules, including nucleotides, proteins, and alkaloids. The process of removing the phosphate group is called dephosphorylation • is present in all tissues throughout the entire body, but is particularly concentrated in liver, bile duct, kidney, bone, intestine and the placenta • isoenzymes: ALPI – intestinal ALPL – tissue-nonspecific (liver/bone/kidney) ALPP – placental (Regan isozyme) • in the liver occurs in the cells lining the biliary ducts • ALP levels in plasma rise with cholestasis (bile duct obstruction, intrahepatic cholestasis, primary biliary cirrhosis, cholecystitis, cholangitis, liver tumor, liver metastases), or infiltrative diseases of the liver (cirrhosis, hepatitis, fatty liver, sarcoidosis, drug intoxication - e.g. verapamil, carbamazepine, phenytoin, erythromycin, allopurinol, ranitidine)
Alkaline phosphatase (ALP) • ALP is also present in bone, and placental tissue, so it is higher in growing children (as their bones are being remodelled), elderly patients with Paget's disease and in many more causes (e.g. osteosarcoma, bone metastases of prostatic cancer, other bone metastases, renal osteodystrophy, fractured bone, multiple myeloma (only when associated with fractures), osteomalacia, rickets, vitamin D deficiency). In the third trimester of pregnancy, ALP is about two to three times higher. • If it is unclear why alkaline phosphatase is elevated, isoenzyme studies using electrophoresis can confirm the source of the ALP. • ELFO: commonly only 2 fractions: α2 (liver -52%) a β1 (bone -48%), after the 16th week of pregnancy placental intestinal: only in blood group A or 0 in plasma, it binds to ery blood group A RR: 20 to 140 IU/L, FN Motol 0,66 – 2,2 μkat/L
Gamma glutamyl transpeptidase (GGT) • also called gamma-glutamyl transferase • it is an enzyme that transfers gamma-glutamyl functional groups • it catalyzes the transfer of the gamma-glutamyl moiety of glutathione to an acceptor that may be an amino acid, a peptide or water (forming glutamate) • this general reaction is: (5-L-glutamyl)-peptide + an amino acid peptide + 5-L-glutamyl amino acid • It plays a key role in the gamma-glutamyl cycle, a pathway for the synthesis and degradation of glutathione and drug and xenobiotic detoxification. • It can also exert a prooxidant role, with regulatory effects at various levels in cellular signal transduction and cellular pathophysiology. • It is found in the cell membranes of many tissues, the most notable are the liver and bile duct, other tissues are: the kidneys, pancreas, gallbladder, spleen, heart, brain, and seminal vesicles. • It is involved in the transfer of amino acids across the cellular membrane and leukotriene metabolism.
Gamma glutamyl transpeptidase (GGT) • GGT is predominantly used as a diagnostic marker for liver disease, latent elevations in GGT are typically seen in patients with chronic viral hepatitis infections often taking 12 months or more to present • Elevated GGT can be found in diseases of the liver, biliary system, and pancreas.It is similar to ALP in detecting disease of the biliary tract (these two markers correlate well, the main value of GGT over ALP is in verifying that ALP can also be increased in certain bone diseases) • More recently, slightly elevated serum GGT has also been found to correlate with cardiovascular diseases and is under active investigation as a cardiovascular risk marker. GGT in fact accumulates in atherosclerotic plaques. • GGT is elevated by large quantities of alcohol ingestion. Isolated elevation or disproportionate elevation compared to other liver enzymes (such as ALP or ALT) may indicate alcohol abuse or alcoholic liver disease (it may indicate excess alcohol consumption up to 3 or 4 weeks prior to the test). • Numerous drugs can raise GGT levels, including barbiturates, phenytoin, NSAIDs, and aspirin. Elevated levels of GGT may also be due to congestive heart failure. RR: 15-85 IU/L for men, and 5-55 IU/L for women, FN Motol: M 0,14 – 0,84 μkat/L, Ž 0,14 – 0,64 μkat/L
5' Nucleotidase • 5' Nucleotidase (5'NTD) is another test specific for cholestasis or damage to the intra- or extrahepatic biliary system. • In some laboratories, is used as a substitute for GGT for ascertaining whether an elevated ALP is of biliary or extrabiliary origin.
Lactate dehydrogenase (LD, LDH) • LDH is found extensively in body tissues, such as blood cells, liver and heart muscle etc. • it is released during tissue damage a marker of common injuries and disease • A dehydrogenase is an enzyme that transfers a hydride from one molecule to another. LDH catalyzes the conversion of pyruvate to lactate and back, as it converts NADH to NAD+ and back • LD is a protein that normally appears throughout the body in small amounts. Many cancers can raise LD levels, so LD may be used as a tumor marker, but it is not useful in identifying a specific kind of cancer. Measuring LD levels can be helpful in monitoring treatment for cancer. • Noncancerous conditions that can raise LD levels include heart failure,anemia, lung or liver disease… • LD is often used as a marker of tissue breakdown as LD is abundant in red blood cells and can function as a marker for hemolysis. • A blood sample that has been handled incorrectly can show false-positively high levels of LD due to erythrocyte damage.
Lactate dehydrogenase • homo or hetero tetramers composed of M and H protein subunits • The five isoenzymes, each contain four subunits • The major isoenzymes of skeletal muscle and liver, M4, has four muscle (M) subunits, H4 is the main isoenzymes for heart muscle, containing four heart (H) subunits. The other variants contain both types of subunits. H(heart)● M (muscle) ● isoenzymes occurence LD1● ●●●heart,red blood cells, kidney LD2● ● ● ●heart,red blood cells, kidney, reticuloendothelial system LD3● ● ● ● lungs, striated muscle, kidney, reticuloendoth.system, leukocytes LD4● ● ● ●liver, striated muscle,kidney, pancreas,placenta LD5● ● ● ● liver, striated muscle,placenta Usually LD-2 is the predominant form in the serum. A LD-1 level higher than the LD-2 level suggests myocardial infarction (damage to heart tissues releases heart LD, which is rich in LD-1, into the bloodstream). FN Motol RR: 3,5 – 7,0 μkat/l
Lactate dehydrogenase Tissues:A - myocard B - kidneyC - erythrocytesD - lienE - liverF - striated muscleIsoenzymes1 - LD12 - LD2 3 - LD3 4 - LD4 5 - LD5
Bilirubin heme • formerly referred to as hematoidin • it is the yellow breakdown product of normal heme catabolism • it consists of an open chain of four pyrrole-like rings (tetrapyrrole); in heme, these four rings are connected into a larger ring, called a porphyrin ring • heme is found in hemoglobin, a principal component of red blood cells • heme can also come from myoglobin, found mostly in muscle, cytochromes, found mostly in mitochondria, catalase, peroxidase, and nitric oxide synthase • bilirubin is excreted in bile and urine, and elevated levels may indicate certain diseases • it is responsible for the yellow color of bruises, the background straw-yellow color of urine (via its reduced breakdown product, urobilin), the brown color of feces (via its conversion to stercobilin), and the yellow discoloration in jaundice • bilirubin's main physiologic role is as a cellular antioxidant FN Motol RR: 2 – 17 μmol/L
M methyl P propionyl V vinyl
Unconjugated ("Indirect") bilirubin • Erythrocytes generated in the bone marrow are disposed of in the spleen when they get old or damaged. • This releases hemoglobin, which is broken down to heme as the globin parts are turned into amino acids. • The heme is then turned into unconjugated bilirubin in the reticuloendothelial cells of the spleen. This unconjugated bilirubin is not soluble in water, due to intramolecular hydrogen bonding. It is then bound to albumin and sent to the liver.
Conjugated ("Direct") bilirubin • In the liver, bilirubin is conjugated with glucuronic acid by the enzyme UDP-glucuronyltransferase (making it soluble in water) and secreted into the bile by canalicular multispecific organic anion transporter CMOAT (multidrug resistance-associated protein 2 MRP2). Then it goes into the small intestine. • However, 95% of the secreted bilirubin is reabsorbed by the intestines (terminal Ileum) and reaches the liver by portal circulation and then resecreted by the liver into the small intestine. This process is known as enterohepatic circulation. FN Motol RR: 0 – 5 μmol/L
Conjugated ("Direct") bilirubin • Conjugated bilirubin is than metabolised in the large intestine by colonic bacteria to form urobilinogen, which may be further oxidized to urobilin. Urobilinogen can be directly reduced to stercobilin. Urobilinogen can also be reduced to stercobilinogen, and further oxidized to stercobilin. • Urobilin, stercobilin and their degradation products give feces its brown color. Thus, having white or clay-colored stool is an indicator for a blockage in bilirubin processing and thus potential liver dysfunction or cholestasis. • However, just like bile, some of the urobilinogen is reabsorbed and 95% of what is reabsorbed is resecreted in the bile which is also part of enterohepatic circulation. • A small amount of the reabsorbed urobilinogen (about 5%) is excreted in the urine following further oxidation to urobilin which gives urine its characteristic yellow color. • This whole process results in only 1–20% of secreted bile being lost in the feces. The amount lost depends on the secretion rate of bile.
Bilirubin • Although the terms direct and indirect bilirubin are used equivalently with conjugated and unconjugated bilirubin, this is not quantitatively correct. • The direct fraction includes both conjugated bilirubin and δ bilirubin(bilirubin covalently bound to albumin, which appears in serum when hepatic excretion of conjugated bilirubin is impaired in patients with hepatobiliary disease- cholestasis). • Measurement of total bilirubin includes both unconjugated and conjugated bilirubin. • Addition of high-concentration hydrophobic drugs (certain antibiotics, diuretics) and high free fatty acids can cause elevated unconjugated bilirubin.
Increased total bilirubin (TBIL) causes jaundice, and can indicate a number of problems: • Prehepatic: increased bilirubin production can be due to a number of causes, including hemolytic anemias and internal hemorrhage • Hepatic:problems with the liver are reflected as deficiencies in bilirubin metabolism (reduced hepatocyte uptake, impaired conjugation of bilirubin, and reduced hepatocyte secretion of bilirubin) Some examples would be cirrhosis and viral hepatitis. • Posthepatic:obstruction of the bile ducts is reflected as deficiencies in bilirubin excretion (Obstruction can be located either within the liver or in the bile duct) Jaundice may be noticeable in the sclera of the eyes at levels of about 2 to 3 mg/dL (34 to 51 μmol/L), and in the skin at higher levels. 1 mg/dL = 17.1 µmol/L
Direct bilirubin • The diagnosis is narrowed down further by evaluating the levels of direct bilirubin. • If direct (conjugated) bilirubin is normal, then the problem is an excess of unconjugated bilirubin (indirect bilirubin), and the location of the problem is upstream of bilirubin conjugation in the liver. Hemolysis, viral hepatitis, or cirrhosis can be suspected. • If direct bilirubin is elevated, then the liver is conjugating bilirubin normally, but is not able to excrete it. Bile duct obstruction by gallstones or cancer should be suspected.
Congenital bilirubin disorders • About 5% of the population has Gilbert's syndrome, a mutation (or variation) in the UDP-glucuronyl-transferase that manifests itself as jaundice when the individual is stressed (i.e. starves). • Autosomal recessive knockouts of UDP-glucuronyl-transferase can lead to Crigler-Najjar syndrome (often leads to brain damage in infants) and elevations of unconjugated bilirubin. • Defects in CMOAT (MRP2) results in Dubin-Johnson syndrome (autosomal recesive disorder, it is usually asymptomatic but may be diagnosed in early infancy based on laboratory tests) and elevations of conjugated bilirubin. • Rotor syndrome is a rare, relatively benign autosomal recessive bilirubin disorder. It is a distinct, yet similar disorder to Dubin–Johnson syndrome — both diseases cause an increase in conjugated bilirubin.
High bilirubin in neonates • Neonates are especially vulnerable to high unconjugated bilirubin levels due to an immature blood-brain barrier that predisposes them to kernicterus/bilirubin encephalopathy (bilirubin accumulates particularly in the basal nuclei), which can result in permanent neurological damage with seizures, abnormal reflexes and eye movements etc. • Neonates also have a low amount of functional UDP-glucuronyl-transferase and can have elevated unconjugated bilirubin, since conjugated is limited. • Neonates in general are at increased risk since they lack the intestinal bacteria that facilitate the breakdown and excretion of conjugated bilirubin in the feces (this is largely why the feces of a neonate are paler than those of an adult). Instead the conjugated bilirubin is converted back into the unconjugated form by the enzyme β-glucuronidase (in the gut, this enzyme is located in the brush border of the lining intestinal cells) and a large proportion is reabsorbed through the enterohepatic circulation.
High bilirubin in neonates • So, newborns are often treated with UV light to turn the hydrophobic, albumin-binding unconjugated bilirubin into a form that is more hydrophilic and able to be secreted in urine, sparing the neonate's brain. • Some of the double-bonds in bilirubin isomerize when exposed to light. This is used in the phototherapy of jaundiced newborns: the E,Z-isomers of bilirubin formed upon light exposure are more soluble than the unilluminated Z,Z-isomer, as the possibility of intramolecular hydrogen bonding is removed. This allows the excretion of unconjugated bilirubin in bile.
Coagulation test • The liver is responsible for the production of coagulation factors. • INR (international normalized ratio) measures the speed of the extrinsic pathway of coagulation, comparing it to normal. • Increased levels of INR means blood is taking more time than usual to clot. • The INR increases only if the liver is so damaged that synthesis of vitamin K-dependent coagulation factors has been impaired; it is not a sensitive measure of liver function. • It is used to determine the clotting tendency of blood, in the measure of warfarin dosage, liver damage, and vitamin K status. • It measures factors I (fibrinogen), II (prothrombin), V, VII, and X. • APTT (activated partial thromboplastin time)is a performance indicator measuring the efficacy of both the "intrinsic" and the common coagulation pathways. Apart from detecting abnormalities in blood clotting, it is also used to monitor the treatment effects with heparin, a major anticoagulant.
Serum glucose • The serum glucose test measures the liver's ability to produce glucose (gluconeogenesis). • It is usually the last function to be lost in the setting of fulminant liver failure.
Metabolism of saccharides • glucostatic function of the liver • glycogen synthesis, glycolysis • glycogen degradation, gluconeogenesis • glucokinase, glc-6-phosphatase • pentose cycle • Cori cycle and glucose-alanine cycle • excess of glucose FFA TAG • transformation of saccharides to glucose • metabolism of fructose (fructokinase) • synthesis of amino saccharides • synthesis of uronic acids • degradation of insulin and glucagon
Metabolism of lipids • liver controls blood FFA concentration • energy is produced mainly by b-oxidation • synthesis of ketone bodies • synthesis of TAG (from FFA, glc, AA) • synthesis of cholesterol • synthesis of bile acids • synthesis of phospholipids • synthesis of VLDL and HDL • degradation of plasma lipoproteins
Metabolism of N-containing compounds • synthesis of plasma proteins (except Ig) • synthesis of coagulation factors • synthesis of acute phase reactants • degradation of amino „N“ (urea, Gln) • synthesis of nonessential amino acids • metabolism of aromatic AAs • degradation of purines to uric acid • synthesis of creatine • conjugation and excretion of bilirubin