Download
1 / 15
150 likes | 320 Vues
Epidural Bleed with a Blunt Carotid Injury. R. Todd Maxson, M.D. Trauma Medical Director John Recicar, RN Nursing Director Trauma Center Arkansas Children’s Hospital. Pre-hospital. 16 year old female previously healthy, high speed rollover Combative on scene and not moving left side

E N D
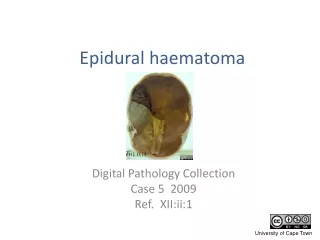
Epidural Bleed with a Blunt Carotid Injury R. Todd Maxson, M.D. Trauma Medical Director John Recicar, RN Nursing Director Trauma Center Arkansas Children’s Hospital
Pre-hospital • 16 year old female previously healthy, high speed rollover • Combative on scene and not moving left side • Intubated on Scene • Rapid transport to Level III TC
Initial Hospital • Evaluation at OSH • To OR for evacuation of Epidural • Specialized transport team requested
Transport • Team met patient in PACU • Optimized ventilation • Started a Transfusion • Returned to ACH
Tertiary Center • Direct admit to PICU • Involved Pediatric Surgery, CCM, Neurosurgery and Vascular Surgery • MRI / MRA done to evaluate brain injury and carotids with non resolved left sided discrepancy in movement
Injuries • Pulmonary contusions • Epidural with a shift • Carotid dissection with pseudoaneurysm • Occipital condyle fracture
Tertiary Center • Quickly extubated and transferred out of ICU • Duplex ultrasound– unable to visualize lesion • Aspirin for anti-platelet effect followed by TEG • Lovenox at 60 mg BID for prevention of thrombin conversion with anti Xa level
Tertiary Care • Admitted to Rehab service on day 4 with discharge on day • Continued on Warfarin • Ultrasound study – no change in lesion • Follow up with ultrasounds and Vascular Surgery
Why use TEG • Demonstrates all phases of hemostasis • Initial fibrin formation • Fibrin-platelet plug construction • Clot lysis • Identifies imbalances in the hemostatic system • Risk of bleeding • Risk of thrombotic event • Allows for individualization of component replacement
Remaining Questions • When and How to screen for carotid injury • What is the appropriate early treatment • TEG use and level of inhibition • Definitive treatment • Stent • Long term anticoagulation - ?
Should the transport team fully optimize before leaving? • Yes – to prevent hypotension and hypoxia following TBI • Maybe – depends on how sick the child is or if a critical intervention is needed • No – doesn’t make a difference
What do routine lab test of anticoagulation (PT, APTT) lack that TEG provides? • Ignore altered thrombin generation • Ignore cellular elements • Ignore overall clot structure • All of the above