Download
1 / 86
860 likes | 1.11k Vues
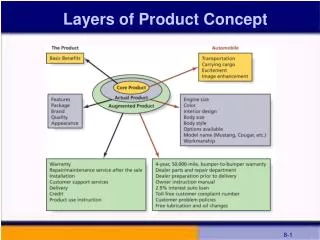
A Product/Business Development Case Study ‘ Identifying Retiree Healthcare Issues & Business Opportunities’. Confidential. Presented by: Westport Consulting Group, Inc. 140 Water Street South Norwalk, Connecticut 06853 203-866-6200 www.westportconsulting.com. Workshop Objectives.

E N D
A Product/Business Development Case Study‘Identifying Retiree Healthcare Issues & Business Opportunities’ Confidential Presented by: Westport Consulting Group, Inc. 140 Water Street South Norwalk, Connecticut 06853 203-866-6200 www.westportconsulting.com ©2003Westport Consulting Group, Inc.
Workshop Objectives • To outline a proven new business/product development process. • To illustrate this process using a real-life project study from the healthcare industry. • To demonstrate various research techniques that go beyond the obvious. ©2003Westport Consulting Group, Inc.
Caveats • We will protect the confidentiality of the client whose work is being discussed today. • We are not trying to force a point of view with the data, but feel it is more useful to illustrate a process with real observations, findings and conclusions that are relevant to this conference. • The facts and conclusions represented in this case study are 4 years old and have not been updated. • However, some of the observations, while widely accepted today, were nascent concepts in 1998. ©2003Westport Consulting Group, Inc.
Important Takeaways From Today’s Workshop • Focus Groups do not equal market research. • There are few if any truly ‘proprietary’ ideas within healthcare and financial services…and if there are they are easily copied. • If you can observe something within the marketplace, so can your competitors. • Don’t assume your competitors are any less competent than yourself. • A compartmentalized development process reduces risk as you go to market. • Don’t be afraid to walk away from a good idea that can’t be objectively validated. • If it was easy or ‘risk free’ everyone would have already done what it is you’re thinking about doing. • Success requires both concept and execution. • Anything and everything can and should be ‘piloted’ before roll-out. ©2003Westport Consulting Group, Inc.
Case Study Project’s Objectives • Examine current commercial retiree health benefit market. • Dimension the commercial retiree health benefit decision-making process and purchase decision criteria. • Identify opportunities to increase client’s share of and overall effectiveness in the commercial retiree health benefit market. • Recommend ways through which client may proceed… in a controlled fashion… to leverage its brand and insure profitability within the commercial retiree health benefit market segment. ©2003Westport Consulting Group, Inc.
Start With A Project Plan • Gets everyone on the same page. • Manages expectations. • Defines and compartmentalizes deliverables. • Suggests proper sequencing. • Avoids “research for research’s sake.” Insist on multiple validation points. Don’t be afraid to stop to measure progress. ©2003Westport Consulting Group, Inc.
Go/No Go Retiree Product Line Market Sizing & Customer Analysis Project Plan Phase II - 6 to 8 weeks 7. Quantitative research (projectible to client corporate market universe) to validate key marketing assumptions PROJECT START 5. Minimum of 4 focus groups (designed to bracket relevant markets) with senior HR and Benefits corporate decision makers to explore decision making process & behavior, exposing and gaining insights into potential new product, positioning, pricing and promotional opportunities for client 9. Creation of comprehensive spreadsheet model to test all assumptions against client ROI/ROE objectives including the sizing of the commercial retiree market 6. Refinement & review of potential client program opportunities based on research findings 1. Extant scan of all related literature client documents & research Go/No Go 8. Analysis & internal research to validate key operational assumptions 2. Two days of structured phone interviews with sample of current client retiree benefit sponsors 2. Internal work session with client Commercial Retiree Team 3. Synthesis of all data & creation of working set of operating hypotheses for client Retiree sponsorship 10. Based on model, the creation of formal Business & Marketing Implementation Plans Phase III - Task 11= 1-2 weeks 11. Creation of internal capabilities, staffing, training, legal and operational requirements Phase I - 4 weeks 12. Pilot to test/validate marketing plan and operational implementation Go/No Go Phase IV TBD 13. New Program ROLL-OUT ©2003Westport Consulting Group, Inc.
Secondary Research Findings ©2003Westport Consulting Group, Inc.
PROJECT START 1. Extant scan of all related literature client documents & research ©2003Westport Consulting Group, Inc.
Why Did We Go To The Trouble Of Looking At Stuff That Everyone ‘Knows’? • It’s almost free. • It’s typically well organized. • It helps you focus. • It keeps you from reinventing the wheel. • It makes you smart enough to approach experts. • It clarifies what you ‘don’t know’. • It codifies ‘conventual wisdom’. ©2003Westport Consulting Group, Inc.
How Do You Properly Find & Obtain Secondary Data? • Turn your client inside/out. • Web searches. • Literature databases. • Trade Associations. • Governmental Bodies, Commissions, Committees & Panels. Secondary research searching and analysis is a specialized skill. ©2003Westport Consulting Group, Inc.
Workplace Dynamics First Drove Demand for Retiree Health Coverage 1950’s – 70’s • “Cradle-to-Grave” employment philosophy. • “Fringe” benefits used to attract talent – “tax-effective compensation.” • Low cost of retiree health care. • High “active-to-retiree” employment ratio. • Comprehensive medical benefits offered to retirees. • Primarily an indemnity health insurance model. • Retiree health insurance cost expensed as incurred. ©2003Westport Consulting Group, Inc.
Changing Workplace Dynamics Have Now Altered theEmployer’s Response to Retiree Health Coverage 1980’s – 90’s • Corporate downsizing takes hold – more expensive employees out placed and skewed to older employees. • Baby Boomers near retirement – accelerated by “right-sizing.” • Outsourcing as a workforce alternative grows to become an acceptable labor management practice. • FASB 106 exposes exploding liability of retiree health coverage cost for large employers. • Rapid acceleration of technology and processes designed to increase productivity are introduced in a concerted effort to reduce growth in FTE. • Migration toward managed care to contain rapid increase in healthcare costs. ©2003Westport Consulting Group, Inc.
The Employer’s Paradigm Has Reserved Itself From The “Cheap” People of the Past to “Expensive” People Today. High Technology 1950’s to Mid 1980’s Cost to Employer $ People Low People High Cost to Employer $ Technology Mid 1980’s to Present Low ©2003Westport Consulting Group, Inc.
Most Active Employees Are Expected To Contribute To Their Healthcare Coverage Employee Pays All 2% Company Pays All 5% Company Pays All But Deductible 10% 79% Company Subsidizes % Distribution of Employer/Employee Health Cost Sharing Source: WCG, Inc. Quantitative Survey of Retiree Health Benefit Decision Makers At Mid and Large Employers 3/98 ©2003Westport Consulting Group, Inc.
Historically, Healthcare Cost Per Active Employee Grew Until Retirement ...Then Diminished Substantially Historical View Employer Cost $ Medicare Employer Cost $ Retiree: MediGap Coverage MediSup Coverage Employer Sponsored Health Coverage Age 25 Age 65 “Normal Retirement” ©2003Westport Consulting Group, Inc.
However, Changing Workplace Practices Have Created A “Second” More Expensive Phase of Healthcare Costs For Those Individuals Who Have Left the Active Workforce But Are Not Yet Medicare Eligible Conceptual View Typically About Age 55 Retired Non-Medicare Eligible Age 65 Medicare Eligible Age 25 Active ©2003Westport Consulting Group, Inc.
Concurrently, Employer Sponsored Costs For Retiree Healthcare Coverage Have Also Continued to Rise $3,182 $3,131 $2,859 $2,751 $2,548 Source: National Survey of Employer Sponsored Health Plans 1997, Forster Higgins & Co. ©2003Westport Consulting Group, Inc.
And, Average Annual Costs Per Cobra Participant Demonstrate That Employers Are Subsidizing The Claims Costs Of Continued Coverage (Mostly For Older, Non-Medicare Eligible Individuals) By An Average of 30% $5,844 $5,703 $5,399 $5,301 $4,307 $4,206 $3,854 $3,903 $3,710 $3,420 $2,852 $2,769 Active Employee Cobra Source: Charles D. Spencer & Associates, Inc. ©2003Westport Consulting Group, Inc.
And, With An Ever Increasing Pool of Non-Medicare Eligible Retirees, The Trend For Employer Funding Of All Of These Benefits Is Declining 24% 19% 18% 17% 20% 17% 13% 16% % of Employers Paying All Benefits 9% 6% Employer Pays All < 65 Employer Pays All 65+ Source: U.S. Department of Labor, Bureau of Labor Statistics, “Employee Benefits in Medium and Large Firms, 1988 and 1989, “Employee Benefits in Medium and Large Private Establishments,” 1991, 1993 and 1995 ©2003Westport Consulting Group, Inc.
Laying A FoundationCreating A Working Hypotheses ©2003Westport Consulting Group, Inc.
2. Two days of structured phone interviews with sample of current client retiree benefit sponsors 2. Internal work session with client Commercial Retiree Team ©2003Westport Consulting Group, Inc.
Why Did We Conduct Interviews With Clients First? • Never trust the client. • Don’t re-invent the wheel. • Check to your secondary research observations. • Understand client’s/market’s constraints early in the process. • Start with people who want to help you. Never conduct an interview without a guide and a purpose. Two people are always better than one. ©2003Westport Consulting Group, Inc.
Preliminary Explorations With Current Commercial Retiree Healthcare Clients Introduction Who we are What we want Understanding what you do Tell me about your current products What do you offer? Why those? How well do they work? ©2003Westport Consulting Group, Inc.
How is it that you became specifically involved with our client? • Tell me about your relationship with my client. • How did you decide to become involved with this healthcare firm? • Walk me through the process, if you can Who initiates? Who is involved? Who has what tasks? Who is vital and who is just helpful? Who does the real homework? Who has the ability to say “no”? Who can say “yes”? ©2003Westport Consulting Group, Inc.
Now that you have a vendor relationship with our client, how do you go about evaluating new concepts and products? Please help me understand how you decide to become involved: Who initiates? Who is involved? Who has what tasks? Who is vital and who is just helpful? Who does the real homework? Who has the ability to say “no”? Who can say “yes”? ©2003Westport Consulting Group, Inc.
Qualitative Research FindingsBuilding On Working Hypotheses ©2003Westport Consulting Group, Inc.
5. Minimum of 4 focus groups (designed to bracket relevant markets) with senior HR and Benefits corporate decision makers to explore decision making process & behavior, exposing and gaining insights into potential new product, positioning, pricing and promotional opportunities for client ©2003Westport Consulting Group, Inc.
Why Did We Choose To Conduct Focus Groups? • Fastest way to expand our view of the market. • Power of a group to build upon preliminary ideas. • Appropriate way to prioritize our observations through the eyes of the market. • Sharing information on retiree benefits among the respondents was seen as a plus not a minus. • In-depth probing not required. Don’t use the session to gather data otherwise available. Always remember that observations are directional not projectable. ©2003Westport Consulting Group, Inc.
Other Qualitative Research Options • In-depth personal interviews. • In-depth telephone interviews. • Dyads and Triads. • Net Meetings. Target your technique to your need, audience and budget. ©2003Westport Consulting Group, Inc.
Discussion Guide:Focus Groups Warm up (estimated time: 10 minutes) Introduce selves: names, companies (if not by name then in-profile so participants can better frame each other’s comments), titles, current and past experience with making health insurance decisions Present overview of focus group: no right or wrong answers, please answer only for yourself not for what "others" might think, no bad answers are possible, you are the expert on you, etc Explain Committed Response procedure: write down number 1-10 on pad for each idea and a few words to remind yourself of why you wrote that down; then we discuss your opinions Topic being discussed: how you go about making decisions about health insurance for your retired workers. Understanding current coverage(estimated time: 20 minutes) Please describe your current health care coverage for retirees. Is it the same for all retirees? Is it the same for current employees? If not, what are the differences? Why are such differences put into place? Relationships with the managed health care companies or insurance carriers who provide this care: (Note: care will be taken to keep comments factual, preventing any individual company “bashing.”) Who provides care? For how long have they been in place? Who was there before? Why current carrier/supplier? Why did you change? Are there some carriers/suppliers who seem better suited for this task than others? Which ones? Why? ©2003Westport Consulting Group, Inc.
Evaluating new concepts and products: the process (estimated time: 25 minutes) (Note: Absent of any “new” concepts, the client’s current products can be introduced on a “no-name/generic” basis to provide a starting point for the group’s consideration.) Please think back as to the last time you considered this topic; it may be when you changed coverage, decided not to change coverage, or might simply have been deciding whether to add or drop coverage. Please walk me through the process: How is the process initiated? Why is it initiated? Which departments are involved? Which areas do which tasks? How long does this take? How are key data obtained? Are there any outside players? Who? What do they do? What checks and controls exist? What inputs are desirable? What ones are necessary? What is the desired final result? Realistically, what is the usual result? Is there any basis for establishing the cost? Relative to what measures? Evaluating new concepts and products: the criteria(estimated time: 25 minutes) We just discussed the process. But what are the criteria for judgment? How do you say that this is a better than average or that a worse than average program?: What are the key criteria? What is also desirable but not key? Help me build an “ideal” offering That is the ideal; again, realistically, what is the usual product offering like? How far short of the ideal does it fall? ©2003Westport Consulting Group, Inc.
Evaluating new concepts and products: the players(estimated time: 25 minutes) That’s the process and the product. What about the people? In your organization, who gets involved in the decision making? Who initiates? Who is involved? Who has what tasks Who is vital and who is just helpful? Who does the real homework? Who has the ability to say “no”? Who can say “yes”? Conclusion (estimated time: 10 minutes) Thank you for your help. Before we go...are there companies who you think are well suited to provide this type of program? who? why them? who couldn’t or wouldn’t? why them? Probes: Must they be national? multistate? offer any particular type of policies? why or why not? Any last thoughts? Good bye. ©2003Westport Consulting Group, Inc.
Top Line Findings & Observations • There are strikingly significant differences in behavior between large and small employers. • Pre-Medicare eligible retirees are not recognized as a formal healthcare benefit market segment and are most often perceived as an extension of a company’s active population. • There appears to be no formal set of pre-Medicare retirement healthcare rules to follow, nor recognized “experts” for companies to turn to for guidance. • Young companies and/or companies with high employee turnover simply do not recognize having a retiree healthcare benefit issue. • Apart from the obvious “cost” concerns associated with all benefits, retiree healthcare is not yet a “balance sheet” issue with small to medium size employers, despite FASB 106. ©2003Westport Consulting Group, Inc.
Differences Between Large and Small Employers • Employer concern or focus on retiree healthcare issues is in direct proportion to the actual number of retired employees they have. • Despite the differences in organizational complexity between small and medium size companies, the Human Resource professionals appear to be of equal caliber. • Managed Care is universally recognized as a key ingredient to retiree healthcare cost containment. • Frequently Consultants emerge as advisors to larger companies while brokers appear to be the only outside influence for smaller employers. • Retiree healthcare benefits do not currently have a ‘champion’ either inside or outside most organizations. ©2003Westport Consulting Group, Inc.
Employers Mostly React To Retiree Healthcare Benefits Issues • Events driving retiree healthcare appear to be: • Mergers and acquisitions • Corporate downsizing • Senior executive retirements • First retirements for younger companies • Competitive (benefit initiative) pressures • The impact of changes in Medicare on retiree healthcare benefits appears to be beyond the ability of small to medium size companies to either plan for or predict. ©2003Westport Consulting Group, Inc.
In Most Cases, Pre-Medicare Eligible Retirees Are Not Perceived As A Critical Employee Benefit Population • Active employees are the most important healthcare benefit segment, followed by Medicare-eligible retirees, with pre-Medicare-eligible individuals ranking a distant third. • COBRA is widely viewed as the full extent of company healthcare benefit obligation for involuntary pre-Medicare retirees. • The prevailing trend for retirees appears to lean toward a continuation of whatever healthcare benefits active employees are offered. • When a pre-Medicare healthcare benefit is offered, the company’s financial contribution tends to be capped or reduced. • Excepting some municipal retirees, companies appear to feel the least amount of obligation to the pre-Medicare retired employee population. ©2003Westport Consulting Group, Inc.
Formal Pre-Retirement Healthcare Practices Are Scant • No Human Resource oriented set of guidelines, practices, or rules appears to exist. Current employer behavior is almost entirely “ad hoc.” • Other than COBRA, there are no government regulations of any import. • No national benefits consulting firm identified with topic. • With the possible exception of Kaiser, no managed care provider appears to be focused on the topic. • No public advocacy. ©2003Westport Consulting Group, Inc.
Cost Containment Initiatives Appear To Be More FocusedOn Medicare Eligible Than Non-Medicare Eligible Retirees • Medicare Eligible • Designation of working spouses as “prime” coverage. • Medicare coordinated “carve-outs” to reduce company benefits to be equal to pre-Medicare levels. • Non-Medicare Eligible • Increased employee contribution and/or capped employer contribution. • Some recognition by employers and healthcare providers of age appropriate underwriting/pricing with less subsidy by averaging in younger active employees. ©2003Westport Consulting Group, Inc.
The Decision Making Process For Retiree HealthcareBenefits Is Fairly Uniform • Human Resource managers are both “gatekeepers” and “influencers.” • In all but the largest firms, CEO’s or boards/committees appear to be the decision makers. • Brokers and consultants only influence the healthcare suppliers, not the decision. • Healthcare companies are not sought out directly for any expertise or advice on retiree topics. ©2003Westport Consulting Group, Inc.
Drivers In the Retiree Decision MakingProcess Are Also Fairly Uniform • Cost is always a prime consideration, but measured relative to active employee benefits. • Administration/paperwork issues rank a close second vis-à-vis retiree healthcare. “A good plan is one where no one ever calls me (Human Resources) “I don’t want these people calling me” “Retired people have a lot more time to focus on things like claims” • Dislocating older retirees, from their doctors simply for costs savings, is distasteful and a sensitive issue. • Only major rate increases (>10+%) would cause companies to rebid retiree healthcare contracts; there appears to be a lot of inertia in keeping healthcare plans ‘status quo’. ©2003Westport Consulting Group, Inc.
Issues Surrounding Retiree HealthcarePlan Design Are Universal • Continuity of care. • Good customer (retired employee) service. • Portability of benefits ... preferably within coordinated managed care networks for: – Retirees who move – Retirees who travel • Easy to understand forms and claims procedures. • Tighter coordination of benefits with Medicare. • Age-specific benefits, e.g., wellness, geriatric. • Simplified and unified (actives and retirees) account billing. • However, small employers i.e., < 1000 employee and <100 retirees do not constitute a serious marketing opportunity as the need for special benefit attention is not perceived as compelling. ©2003Westport Consulting Group, Inc.
Retiree Healthcare Opportunities Are Real • Ability to “position” client organization as proactive expert on topic. • Ability to create a defined market segment between commercial and Medicare/HMO • Ability to provide value-added by relieving HR professionals of responsibility and need to create “homegrown” solutions between active and Medicare eligible retirees. • Ability to segment down from strong Medicare/HMO position vs. more generic commercial competitive frame. • Ability to be preemptive in creating, underwriting, and pricing a pre-Medicare retiree pool across company populations. • A focus on pre-Medicare eligible retirees strengthens Medicare/HMO’s new member pipeline. • Targeting of “self-insured” companies to remove or contain expanding retiree liability from their balance sheet. ©2003Westport Consulting Group, Inc.
Program Suggestions In Creating The “Ideal” Retiree Health Plan • Live person telephone assistance (i.e., no VRU or voice mail) • Minimal or no paperwork for employee • Eased access to key specialists • Commitment to established quality service standards that are measurable • Wellness programs • Enrollment exam and personalized healthcare program • Other suggestions included: • Tie-in to long-term care • Tie-in to at-home care • Simplified Rx service • Hospice care • Hearing aid and vision care ©2003Westport Consulting Group, Inc.
Qualitative Group Exercise • Pseudo-Conjoint • Pseudo-Cluster • Pseudo-MDS Rules for Pseudo-MDS Exercise “Characteristics of employee & retiree health plans” Choose your own criteria for difference. Work in as many dimensions as you like. Use the entire room. No two things are exactly the same or completely different. ©2003Westport Consulting Group, Inc.
Quantitative Research FindingsDimensioning Market & Validatingand/or Refining Working Hypotheses ©2003Westport Consulting Group, Inc.
7. Quantitative research (projectible to client corporate market universe) to validate key marketing assumptions ©2003Westport Consulting Group, Inc.
Why Did We Do Quantitative Research? • Establish size of the market. • Generate reliable measure of interest in concepts. • Provide data for effective marketing projection. Survey size is determined by survey objectives. Choosing the “best” product is easy. Determining “how good” is much harder. ©2003Westport Consulting Group, Inc.
Questionnaire BEGIN HERE: Ask to speak with whomever in the company “has senior responsibility for determining where and from whom health insurance is purchased.” A Hello, my name is [____________] from [____________], a market research company. We’re trying to understand how companies like yours handle health insurance for their retirees. This is purely a research study; I assure you, we are not selling anything. Could you please tell me if, other than Medicare, your company has a health insurance program for retirees, either those over 65 or those under 65? Yes, has program for those under 65... 1 (Skip to QC) Yes, has program for those 65 or older... 2 (Skip to QC) Yes, has both... 3 (Skip to QC) No, has neither… 4 Don’t know... 5 (Ask who would know and restart) B. Is your company currently actively and aggressively planning to offer such insurance to your retirees in 1998? (If “yes,” probe for which kind:) Is that for retirees under 65, 65 or older, or both? Yes, for those under 65... 1 Yes, for those 65 or older... 2 Yes, for both over and under 65... 3 No... 4 (Terminate) DK... 5 (Terminate) C. Are you the person in your company who has primary responsibility for determining what kinds of health insurance are offered to your retirees? Yes, am senior person responsible... 1 (Continue) No, but have major inputs... 2 (Check quota) No, somebody else... 3 Ask for referral and restart DK/not sure... 4 Probe/Re-ask question Very roughly, about how many retirees does your company now have? Very roughly, about how many retirees does your company now have? ©2003Westport Consulting Group, Inc.
1. To begin, would you please tell me a few things about the health insurance that is currently provided for active employees. Which, if any, of these types of coverage do you offer? (READ LIST.) Traditional indemnity insurance, with or without deductibles,sometimes called 80/20 insurance... 1 HMOs... 2 PPOs (Preferred Provider networks)... 3 POS (Point of Service networks)... 4 (Do not read:) Other (specify:)__________________ 2. Who pays for that coverage? Would you say that... (READ LIST.) Company pays for all... 1 Company pays for all, except for deductibles and co-payments... 2 Company subsidizes employees but employees pay part... 3 Company provides plan but employee pays for all of it... 4 (Do not read:) Other (explain:)___________________________ IF RESPONDENT OFFERS COVERAGE TO RETIREES UNDER 65, ASK THE FOLLOWING QUESTIONS. OTHERWISE, SKIP TO Q. 11. 3. Would you say that the coverage you offer your under-65 retirees is... Same health benefits as current active employees... 1 Slightly different health benefits as compared to employees... 2 Different health plan benefits than for current employees... 3 4. Who pays the premiums for the these retirees’ health care? Company pays for all... 1 Company pays for all, except for deductibles and co-payments... 2 Company subsidizes employees but employees pay part... 3 Company provides plan but employee pays for all of it... 4 (Do not read:) Other (explain:)___________________________ 5. Which, if any, of these types of coverage do you offer your under-65 retirees? (READ LIST.) T traditional indemnity insurance, with or without deductibles... 1 HMOs... 2 PPOs... 3 POS... 4 (Do not read:) Other (specify:) ©2003Westport Consulting Group, Inc.