Download
1 / 33
380 likes | 911 Vues
pTiO2 en Neuroréanimation G Francony, B Fauvage Équipes Réanimation Neurochirurgicale et Réanimation Polyvalente Chirurgicale CHU de Grenoble. Rationnel. Lésions secondaires ischémiques et pronostic Rôle central de la faillite énergétique: métabolisme aérobie

E N D
pTiO2 en Neuroréanimation G Francony, B Fauvage Équipes Réanimation Neurochirurgicale etRéanimation PolyvalenteChirurgicale CHU de Grenoble
Rationnel • Lésions secondaires ischémiques et pronostic • Rôle central de la faillite énergétique: métabolisme aérobie • Perturbation transport / délivrance O2 • Dysfonction mitochondriale Graham Lancet 1971 Werner Br J anaesth 2007
Perturbation transport O2étape « macrocirculatoire » • Bas débit sanguin cérébral (DSC) • Hypoxie • Anémie Bouma J Neurosurg 1992
Perturbation transport O2étape « microcirculatoire » • Crise métabolique 25% vs ischémie 1-2,4% • ⇑ L/P ratio : HTIC OR = 10 [6-16] Vespa J Cereb Blood Flow Metab 2005 Belli Acta Neurochir 2008
Perturbation délivrance et troubles diffusion Patients stables PtiO2 basse PtiO2 normale hyperventilation Menon Crit Care Med 2004
Demande métabolique accrue • expérimental • Clinique • ↑ Glucose/ oxygen ratio Yoshino Brain Res 1991 Pellerin Magistretti PNAS 1994 Bergsneider J Neurosurg 1997 Vespa J Cereb Blood Flow Metab 2005
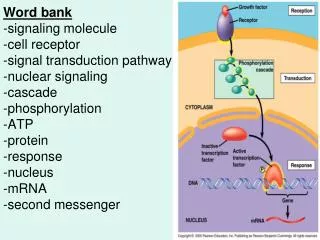
pTiO2 O2 OH- ≈ DDP PtiO2 milieu extra cellulaire cérébral
pTiO2 Hétérogénéité de la vascularisation cérébrale Mesure locale S ≈ 7 à 15 mm2 Dings Neurosurgery 1998
Normalité Pennings J Neurotrauma 2008
↑ PtiO2 avec ↑ PaO2 • Transport en O2 : CaO2 x DSC CaO2 = (SaO2 x Hb x 1,34) + (PaO2 x 0,0003) • Artefact ou réalité? Johnston Br J anaesth 2003
Diringer J Neurosurg 2007 • Augmentation CaO2 • Rôle hématocrite cérébral? • Rôle diffusion McLeod Anesth Analg 2003 Sakai J Cereb Blood Flow Metab 1985 Zauner Neurosurgery 2002
Rosenthal Crit Care Med 2008 • Confirmation • PtiO2 basse: • Problème technique • Bas DSC • Bas Contenu artériel en O2 • Diffusion compromise PtiO2 proportionnelle au produit DSC x (PaO2 - PvO2)
diffusion hypoxie anémie Bas DSC relatif pTiO2 O2 DSC
Pression Tissulaire Cérébrale en Oxygène (PbO2) Durée et profondeur de l’hypoxie van den Brink et al Neurosurgery 2000
Facteur temps Jones J Neurosurg 1981
pTiO2 et DSC Scheufler Anaesthesia Analgesia 2002
Variation de la PbO2 en fonction de la PaO2 par variation de la FiO2 à PAM, PIC, CO2 constants PbO2 (mmHg) N=15 PaO2 (mmHg) Intérêt du rapport PTiO2/PaO2 M. Casez, CHU Grenoble, 2006
Autorégulation Jaeger Crit Care Med 2006
Autorégulation Lang Crit Care Med 2003
Thérapeutique • Optimisation PtiO2/ ⇑ PPC • Optimisation PtiO2 > 25 mmHg/ ⇑ DSC, ⇑ contenu artériel O2, ⇑ diffusion (PaO2) Meixensberger JNNP 2003 Stiefel JNeurosurg 2007
Objectif PtiO2 > 20 mmhg positif négatif Narotam J Neurosurg 2009 AdamidesActa Neurochir 2009 • PIC < 20 mmhg • PPC > 60 mmHg • Hyperoxie • Transfusion
Thérapeutique Brain Trauma recommendations J Neurotrauma 2007
Thérapeutique • en faire assez • mais ne pas en faire trop • pTiO2 !!! 29
? Thérapeutique Eviter survenue de lésions ischémiques secondaires Eviter le développement d’un œdème cérébral Concept de Lund PPC ≅ 50 mmHg Concept de Rosner PPC ≅ 70 mmHg « PPC sur mesure » Cremer, Anesth Analg 2004 Stochetti, Chest 2005 « PCO2 sur mesure » Monitorage du DSC + délivrance O2
PIC < 20 mmHg et PPC > 60 mmHg PIC > 20 mmHg ou PPC < 60 mmHg Pas de traitement Traitement PIC/ PPC (Cambridge, BJA 2007) 2ème ligne: osmothérapie (<320 mOsm/L) hypothermie 35-36°C PaCO2 30-35 mmHg DVE curares PPC >70 mmHg 3ème ligne: craniectomie décompressive thiopental ou propofol pour silence EEG hypothermie <34°C Groupe PIC
PtiO2 > 20 mmHg PtiO2 < 20 mmHg PIC < 30 mmHg PIC > 30 mmHg titration diminution PPC (mini 50 mmHg) Traitement PIC/ PPC Idem groupe PIC PIC < 20 mmHg PIC > 20 mmHg • Optimisation transport O2 • PaO2 100-150 mmHg • PaCO2 35-45 mmHg • Titration augmentation PPC 60-80 mmHg • IC > 2.2 L/min/m2 • Transfusion pour Hb > 10 g/dL • Augmentation FiO2 pour PaO2 >150 mmHg Traitement PIC/ PPC Idem groupe PIC Puis Optimisation transport O2 titration diminution PPC (mini 50 mmHg) ? Pas de traitement Groupe PtiO2 Contrôle PaO2 PaCO2