Download
1 / 38
550 likes | 1.61k Vues
Pre-clinical Periodontics. Dr Jamal Naim PhD in Orthodontics. Gingivitis cont. Puberty associated gingivitis. Appears in both females and males. PD tissue has exaggerated response to local factors Increase in estrogen & progesterone.

E N D
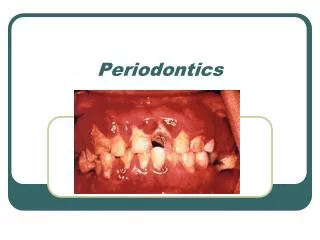
Pre-clinical Periodontics Dr Jamal Naim PhD in Orthodontics Gingivitis cont.
Puberty associated gingivitis • Appears in both females and males. • PD tissue has exaggerated response to local factors • Increase in estrogen & progesterone. • Facial gingiva is enlarged, lingual surface are relatively unaltered. (mechanical action of the tongue & food prevent a heavy accumulation of local irritants on the lingual surface)
Puberty associated gingivitis • Inflamed tissues become erythematous, lobulated & retractable • Easily bleeding with debridement. • Tendency for recurrence during puberty • After puberty the enlargement undergoes spontaneous reduction but does not disappear until local irritations are removed.
Menstrual cycle associated gingivitis • Hormonal imbalances • Increase prevalence of G. • Bleeding and tense feeling in the gingiva • Increased salivary bacterial account • Increase of GCF amount
Pregnancy Gingivitis • Reported in 50-100% of pregnant women. • The same bacterial environment in healthy gingiva pre-pregnancy causes gingivitis during gingivitis • Local irritation starts the condition but the altered tissue metabolism aggravates the response. • Generalized, more prominent interproximal than facial and lingual. • Gingiva is red, soft and friable with spontaneous bleeding • Increases GCF, pocket depth and tooth mobility
Pregnancy Gingivitis • Beginning in the 2nd to 3rd month • Increased severity in the 8th and decrease in the 9th month
pyogenic granuloma/epulis • It is not a neoplasm • Occurs after the 3rd month of pregnancy • Incidence is 1.8 - 5% • Mushroom –like flattened, sessile or pedunculated • Painless unless complicated by inflammation • Very good oral hygiene may prevent enlargement, usually regresses after delivery. • Complete removal requires incision
Diabetes mellitus associated gingivitis Diabetes may be first picked up by the oral health practitioner because of the unusual response of the gingival tissues to plaque.
Diabetes mellitus associated gingivitis • Enlarged red, velvety gingival tissues that bleed easily, • Rapid bone loss / loose teeth, • Multiple periodontal abscesses, • Proliferative granulation tissue at the gingival margin, • Slow resolution of gingivitis after conventional treatment.
Diabetes mellitus associated gingivitis Vascular changes in diabetes: • thickening of the basement membrane of vessel walls leading to reduced: • PMN migration • Oxygen diffusion • Removal of metabolic wastes.
Gingival diseases associated with blood dyscrasias Leukemia associated gingivitis: • Reduced production of RBC, WBC and platelets bu leukemia • True leukemia enlargement occurs with acute rather than chronic leukemia. • Gingiva is shiny, bluish red, firm or friable, may be accompanied by painful necrotizing ulcerative inflammatory involvement. • Areas of Connective tissue infiltrated with dense mass of immature and proliferating leukocytes
Gingival diseases associated with Cyclic neutropenia Cyclic neutropeniais a disorder in which the number of the neutrophils drops dramatically in a cyclical pattern, usually about every 21 days. Very low neutrophil count in Cyclic neutropenia
Gingival diseases modified by malnutrition • Nutritional deficiencies affect the host response to bacterial by-products such as oxygen radicals. • Vitamin C-deficiency (ascorbic acid) –scurvy- is the most known plaque induced gingival disease modified by this malnutrition. • Acute vitamin C deficiency results in edema and hemorrhage in the periodontal ligament and in the gingiva. • Degeneration of collagen fibers • Osteoporosis of the alveolar bone, and tooth mobility. • Impaired gingival healing.
Gingival diseases modified by malnutrition Scurvy - severe Vitamin C deficiency
Gingival diseases modified by malnutrition Scurvy - severe Vitamin C deficiency / 14 year old girl
Non-plaque induced gingival lesions I. Gingival diseases of specific bacterial origin: • Neisseria gonorrheae (gonorrhea) - associated lesions are most common. • Treponema pallidum (syphilis) - associated lesions are lesser common • Streptococcal species (streptococcal gingivitis) -associated lesions are rare.
Non-plaque induced gingival lesions I. Gingival diseases of specific bacterial origin: • Are preceded by tonsillitis • Fever • Pain • Swollen gingiva • Bleeding • Occasionally abscesses
Non-plaque induced gingival lesions II. Gingival diseases of viral origin: • Herpes virus infections • Primary herpetic Gingivostomatitis (most common) • Recurrent oral herpes • Varicella-zoster infections • HIV
Non-plaque induced gingival lesions II. Gingival diseases of viral origin: herpetic Gingivostomatitis
Non-plaque induced gingival lesions II. Gingival diseases of viral origin: Herpes virus-induced acute gingivitis
Non-plaque induced gingival lesions III. Gingival diseases of fungal origin: • Relatively uncommon • By immuno-compromised patients • By long use of broad spectrum antibiotics • Candida-species infections: generalised gingival candidiasis by: • Prosthesis • decreased salivary flow • decreased salivary pH • Increased salivary glucose
Non-plaque induced gingival lesions III. Gingival diseases of fungal origin: generalised gingival candidiasis
Non-plaque induced gingival lesions III. Gingival diseases of fungal origin: • Linear gingival erythema (by HIV) • Histoplasmosis • other Linear gingival erythema
Non-plaque induced gingival lesions IV. Gingival diseases of genetic origin: • Heredity gingival fibromatosis • Me be isolated or associated with generalized syndrms • other
Non-plaque induced gingival lesions IV. Gingival manifestations of systemic conditions: • Mucocutaneous disorders • Lichen planus • Pemphigoid • Pemphigus vulgaris • Erythema multiforme • Lupus erythematosus • Drug-induced • other Lichen planus
Non-plaque induced gingival lesions IV. Gingival manifestations of systemic conditions: • Allergic reactions • Dental restorative materials • Mercury • Nickel • Acrylic (most cold acrylic resin) • other
Non-plaque induced gingival lesions IV. Gingival manifestations of systemic conditions: • Allergic reactions • Reactions attributable to: • Toothpastes/dentifrices • Mouthrinses/mouthwashes • Chewing gum additives • Foods and additives • other
Non-plaque induced gingival lesions VI. Traumatic lesions (factitious, iatrogenic, accidental) • Chemical injury • Physical injury • Thermal injury
Non-plaque induced gingival lesions Tongue jewelry
Non-plaque induced gingival lesions VII. Foreign body reactions • Amalgam • Abrasives during prof. polishing VIII. Not otherwise specified (NOS)