Download
1 / 33
330 likes | 756 Vues
University of Pittsburgh Senior Design – BioE 1160/1161. Redesign of an Intraosseous Needle. Jonathan Hughes Michael Audette Christopher Sullivan April 18, 2006 Mentor: James Menegazzi, Ph.D. The Intraosseous Needle. Intraosseous (IO) needle Access to venous system via IO pathway

E N D
University of Pittsburgh Senior Design – BioE 1160/1161 Redesign of an Intraosseous Needle Jonathan Hughes Michael Audette Christopher Sullivan April 18, 2006 Mentor: James Menegazzi, Ph.D.
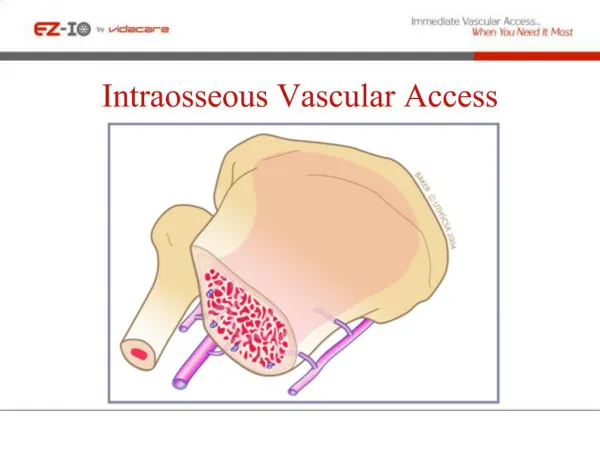
The Intraosseous Needle • Intraosseous (IO) needle • Access to venous system via IO pathway • Components • Needle (14-16 gauge) • Trocar • Plastic housing • Insertion Technique • Placed through cortex • Fluid delivery to marrow • Driven by hand, spring, • or drill action Cook Critical Care, Inc. 2000
IO Access • Major IO Infusion Sites • Pediatric • Proximal tibia (1-5 yrs.) • Adult • Sternum • Tibia (proximal or distal) • Alternate sites • Iliac crest • Distal shaft of the femur Jamshidi IO needle
Proximal Tibia Infusion http://www.vitaid.com
IO Applications • Emergency medicine • Limited access to venous system • Severe burns, trauma, hypovolemic shock, etc. • Fluid and pharmacological resuscitation • Bolus infusion (rapid delivery) • Continuous infusion • Supplemental therapy • Marrow sampling • Clinical settings
Problem Statement • Problem: • Insertion technique and location may result in IO needle occlusion • Requires reinsertion • 15 gauge IO needle redesign: • Facilitate infusion by providing alternate flow paths • Addition of distal side ports • Maintain mechanical strength of needle Occluded IO Insertion
Competitive Analysis • Competitors • Manual insertion • Cook • Jamshidi • Mechanical insertion • EZ-IO (VidaCare) • Bone Injection Gun (WaisMed) • Strengths • Allows the provider to continue to deliver drugs in the event of needle end occlusion • The manual needle, which is our focus, can be used multiple times while spring-loaded devices (i.e., Bone Injection Gun) can only be used once • Weaknesses • With the use of the automatic injection devices, occlusion is not a major problem, although it still happens (~2%)
FDA Regulation Code of Federal Regulations TITLE 21--FOOD AND DRUGS CHAPTER I--FOOD AND DRUG ADMINISTRATION DEPARTMENT OF HEALTH AND HUMAN SERVICES SUBCHAPTER H--MEDICAL DEVICES PART 880 – GENERAL HOSPITAL AND PERSONAL USE DEVICES Subpart F--General Hospital and Personal Use Therapeutic Devices • Sec. 880.5570 Hypodermic single lumen needle. • (a) Identification. A hypodermic single lumen needle is a device intended to inject fluids into, or withdraw fluids from, parts of the body below the surface of the skin. The device consists of a metal tube that is sharpened at one end and at the other end joined to a female connector (hub) designed to mate with a male connector (nozzle) of a piston syringe or an intravascular administration set. • (b) Classification.Class II (performance standards). US Food and Drug Administration: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?FR=880.5570
Project Goals • Redesign a manual 15 gauge intraosseous needle that will allow for continued flow in case of needle tip occlusion (through the addition of distal sideports) • Specific goals • Maintain mechanical stability of the IO needle - CosmosWorks and In vitro testing • If properly inserted, our IO needle should have the same functionality as current IO needles • Capable of delivering 200 cc/min of fluids • If not properly inserted (tip occlusion), our IO needle should still allow for the delivery of meds through the sideports • This additional functionality is not present in current IO needles • Minimize extravasation • Sideports cannot be too far distal - lead to extravasation during occluded infusion • Sideports cannot be too proximal - lead to extravasation during normal infusion
Design Selection Tree How many sideports to add and where? 3+ sets of sideports, 2+ setsof long sideports Addition of Sideports One set of sideports Two sets of sideports Circular Elongated Inline Offset Model A Model C Model B Model D
FEA Testing • Finite Element Analysis testing was done in Solidworks and Floworks • Scenarios to model: • Normal infusion • Occluded infusion (simulated with ideal wall at tip) • Compare models to each other without the need for costly prototype iterations • Allowed for design parameters to easily be changed and retested
Normal Infusion Cut Plot Locations In-hole Flow Trajectories • In normal infusion, ~99% of the flow leaves through the tip (essentially no flow through sideports) • Therefore, during normal infusion, our needle designs function the same as current IO needles Velocity Profile Cutplot (red = higher v) 75 velocity flow trajectories, none leave through the sideports
Occluded Functionality – One sideport – Model A Velocity Profile Cutplot (red = higher v) 75 flow trajectories (velocity) • Heavy backflow (15-20% of overall flow) • High flow velocities out of sideports – could possibly result in hemolysis • Models B and D have more desirable flow patterns • Eliminated
Occluded – One sideport – Model C Velocity Profile Cutplots (red = higher v) 75 flow trajectories (velocity) • Light backflow • Flow profile is similar to Models B and D • Eliminated because Models B and D yield similar results, but are cheaper to manufacture
Occluded – Two sideports – Model B Velocity Profile Cutplots (red = higher v) 75 flow trajectories (velocity) • Light backflow (2-3%) • ~60% of flow out of distal sideport, ~40% out of proximal sideport • Essentially all flow has left the needle by the end of the most distal sideport • Prototyped
Occluded – Two sideports – Model D Velocity Profile Cutplots (red = higher v) 75 flow trajectories (velocity) • Light backflow (2-3%) • Very similar flow profile to Model B • Essentially all flow has left the needle by the end of the most distal sideport • Could be prototyped and compared to Model B (future work)
Prototype • Two prototypes of Model B were produced • Manufactured by Vitaneedle out of 316 Stainless Steel • 316 Stainless steel is the material used in current needles • A Luer Lock hub was attached to the proximal end • The device was modeled to make use of the current Jamshidi needle holder for testing purposes since PIM was not feasible
Constraints limiting testing • Our trocar did not fit properly into the lumen of the needle prototype • Modification of the trocar without compromising tip occlusion was not possible • As a result, direct insertion of our prototype into bone was not feasible • To compensate, a pilot hole using a current needle was first drilled and then our needle was inserted • Our planned in vitro mechanical stability testing was not possible • However, our trocarless hollow needle was hammered into bone to model total tip occlusion and showed no mechanical deformation when removed
Experimental Methods • Flow Rate Determination • Time (in seconds) elapsed to infuse 200 mL of 0.9% saline solution was measured • Steady pressure drop of 275 mm Hg to 300 mm Hg maintained by a pressure infusion bag • Five cases: • Current Jamshidi IO needle (no sideports) without occlusion • Current Jamshidi IO needle with occlusion • Redesigned IO needle without occlusion • Redesigned IO needle with occlusion from rubber stopcock • Redesigned IO needle with simulated occlusion in distal end of porcine tibia bone cortex • 10 Trials of each case
Discussion of Results • Over 10 trials, our redesigned IO needle was able to deliver ~300 cc/min of fluid in the event of both cases of tip occlusion • Very similar to non-occluded cases • 300 cc/min more than adequately satisfies our baseline goal of 200 cc/min • Therefore, there appeared to be virtually no difference in infusion time of 200 mL of fluid • Obviously, when the tip is occluded in the current IO needle (without sideports), flow is blocked, and there is no path for infusion • In the case of the non-occluded needle with sideports, we noticed that all flow passed through the open end even with the sideport openings • Minimal Extravasation
Testing (con’t) • Dr. Menegazzi used our prototype in testing a deceased porcine test subject • The result was that there happened to be needle tip occlusion inadvertently, but aspiration still took place • This shows that the sideports provided an alternate path for fluid flow
Human Factors • Device does not require the device user population to be highly skilled in needle operation techniques • Training with device will consist of the formal training that is standard to normal intraosseous needle use • Familiarization of users with the slight differences between the new design and current products of which the users already have experience using • Device will be used in the field in emergency care and thus may be used in any location • Hospitals • Stationary and or Moving Vehicles (i.e., ambulances)
Acknowledgements • James Menegazzi, PhD • Steven Abramowitch, PhD • VitaNeedle • University of Pittsburgh Department of Bioengineering • Generous donation from Drs. Hal Wrigley & Linda Baker • Mark Gartner
Questions ???