Books...Books...Books...
720 likes | 1.03k Vues
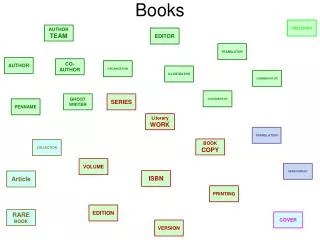
Books...Books...Books. Robbins Basic Pathology Editörler: Vinay Kumar, Abul K. Abbas, Nelson Fausto ISBN: 9780808923664 Türkçesi: Robbins Hastalığın Patolojik Temeli - ISBN 9789752771802 Robbins Temel Patoloji – ISBN: 9781416029731

Books...Books...Books...
E N D
Presentation Transcript
Books...Books...Books... • RobbinsBasicPathology • Editörler: Vinay Kumar, Abul K. Abbas, Nelson Fausto • ISBN: 9780808923664 • Türkçesi: • Robbins Hastalığın Patolojik Temeli - ISBN 9789752771802 • Robbins Temel Patoloji – ISBN: 9781416029731 • RobinsReview of Pathology (Türkçesi) -ISBN :975-8531-21-2 • Rubin'sPathology: ClinicopathologicFoundations of Medicine • Editör(ler) :RaphaelRubin , David S Strayer • ISBN :0781795168 • EssentialPathology • Editör:EmanuelRubin • ISBN :0781723957 • Temel Patoloji • Editör:Prof. Dr. Gamze Mocan KUZEY • ISBN :975-277-104-1
All tissues in the body are composed of • parenchymal cells, which are specialized to perform the functions of that particular tissue, • interstitial connective tissue elements, which act as the supporting framework of the tissue. • Human disease results from the action of various injurious agents on tissues.
The normal cell is confined to a fairly narrow range of function and structure by its • genetic programs of metabolism, • differentiation, • specialization. • More excessive physiologic stresses or some pathologic stimuli a number of physiologic and morphologic cellular adaptations. • If the limits of adaptive response to a stimulus are exceeded, or in certain instances when adaptation is not possible, a sequence of events follows, loosely termed cell injury.
Structural damage • Interstitial tissue damage • Parenchymal cell damage • reversible change (cell degeneration) • irreversible cell death (cell death; necrosis). • interstitial abnormalities.
Direct Injury • A noxious agent may act directly on the tissue • burn • Indirect Injury • An injurious agent may act at some site other than the tissue in question to produce an abnormality. • accumulation of toxic products in kidney and liver failure • change in extracellular pH, electrolyte concentrations, or core body temperature.
PHYSICAL INJURY • MECHANICAL TRAUMA • PRESSURE INJURIES • INJURIES due to HEAT & COLD • ELECTRICAL INJURIES • RADIATION INJURY
Principles of Cell Injury Cell injury dependents upon: • the etiology, • duration, • severity of the inciting injury • cell type, • stage of cell cycle, • cell adaptability. Morphologic reactions occur only after critical biochemical (molecular) damage.
The Pathology of Cell Injury DEGENERATION NECROSIS
1. DEGENERATION Reversible cell injury has two morphologic hallmarks: • cell swelling • fatty change
Hydropic swelling ("cloudy swelling“) • The visible change resulting from water being pulled by osmosis through damaged cell membranes is due to acute injuries • The extreme forms are called "vacuolar degeneration" • Hydropic swelling is an increase in cell volume characterizedby a large, pale cytoplasm and a normally located nucleus.
Fatty change • Occurs when cells which ordinarily take up a lot of lipid (liver) cannot process it.
Functional and morphologic consequences of decreased intracellular ATP during cell injury
Reversible injury (EM) • Plasma membrane blebs • Dissociation of ribosomes • Swollen mitochondria • Aggregation of nucleolus
General Biochemical Mechanisms • Defects in volume regulation – reversible • ATP depletion or interference with production • Increased permeability to sodium (Na+) • Oxygen free radical damage to the membrane or its Na-K ATPase sodium pump • Necrosis – irreversible • Loss of calcium homeostasis • Membrane defects • Mitochondrial damage (calcification – dense bodies)
Cell death • Necrosis is the death of cells prior to the death of the organism, and its visible (grossly and/or microscopically) evidence. • The ultimate result of cell injury.
Hypoxia (lack of oxygen), • Infection (viruses explode cells when they multiply), • Toxins (endo&exo, poisons, metals, ect.), • Immune reactions (autoimmune antibodies).
Hypoxia • Loss of the ability to carry on sufficient aerobic oxidative respiration, is the most common cause of cell injury and death. • It is the prototype cause of the cell Degeneration & Necrosis.
Etiology of Hypoxia • 1.Ischemia(ischemic hypoxia; stagnant hypoxia): Loss of arterial blood flow • 2. Hypoxemia: Blood problems- too little oxygen in the blood • 2.1. Anemichypoxia: Hemoglobin problems • Inadequate circulating red cell mass (anemia) • Inability of hemoglobin to carry the oxygen (carbon monoxide poisoning)
2.2. Hypoxic hypoxia:Oxygen and/or ventilation problems • 3. Histotoxic hypoxia:Failure of the cytochromes • Cyanide poisoning • Rotenone poisoning • Dinitrophenol poisoning • Other poisons. Of course, increased metabolic demands (exercise, fever) will exacerbate any of these problems.
What happens during Hypoxia ? Hypoxia cell can't do oxidative phosphorylation glycolysis increases greatly lactic acid builds up drops the cell pH proteins denature.
This lets: • water, sodium andcalcium into, • potassium and various marker enzymes out of, the cells. • Water-and-lipidphases separate as layers • The cell andits endoplasmic-reticulum may swell with water (hydropicswelling) This isdegenerationand isstill reversible.
When hypoxia is bad enough, thecalcium precipitates the phosphates in the mitochondria (mitochondrialdensities) which kills the cell. • Membrane injury is irreversible. • Lysosomes may burst, and free fatty acidscan act as detergents.
The hallmark of early irreversible hypoxic injury is "calcification of the mitochondria". • Hypoxia • i ATP i • i Ion pumps cell swelling • Glycolysis ipH lysosome breakdown • Disruption (synthesis/storage) • Membrane injury lysosome breakdown • Enzyme escape + Calcium influx
Nuclear changes • Pyknosisis a shriveling and darkening of the nucleus attributed to very low pH. • Later stages include • Karyorrhexis, or fragmentation of the shriveled nucleus into nuclear dust, • Karyolysis, which simply means that nothing of the nucleus is visible any longer, except perhaps a purple haze.
Reperfusion injury When blood flow is restored; this also results with injury • Reperfusion • membrane injury • lysosome breakdown • free radicals • enzyme escape + calcium influx.
Neurons (Ex: cells of brain and all nervous system) undergo frank necrosis after being deprived of oxygen for 3-5 minutes at normal temperature (and clinically, brain damage follows much shorter intervals). • Heart muscle cells can last for30-60 minutes. • Liver cells and renal tubular cells can last for 1-2 hours without oxygen • Skeletal muscle cell can last forsix hours.
NECROSIS The death of cells prior to the death of the organism, and its visible (grossly and/or microscopically) evidence. • Autolysis: is the dead cell being self-digested by its lysosomal enzymes. • Heterolysis: is the cell being digested by the body's living white cells. • Putrefaction is the lysis of dead tissue (part of a live body, or a dead body) by bacterial enzymes, producing nasty smells.
Coagulation necrosis Liquefactive necrosis Caseous necrosis Gangrene Enzymatic fat necrosis Gummatous necrosis Fibrinoid necrosis Types of Necrosis
Coagulation necrosis • Death of groups of cells (most often from loss of blood supply- ischemia), with persistence of their shapes for at least a few days. • Myocardial infarction is a typical Coagulation necrosis of the heart muscle.
Grossly, the dead area is likely to be soft and pale. • After a while, it is likely to shrink (catabolism) and turnthe yellow color.
Liquefactive necrosis • Colliquative (colliquation) necrosis(Turkish=erime nekrozu) • The result of hydrolysis (autolysis or heterolysis) • When the cells die, they are rapidly destroyed by lysosomal enzymes: • either their own or those from neutrophilic leukocytes (i.e., bacterial infections) • clostridia • snake poison.
Acid and alkaline burns represent the extreme of liquefaction. • Also, if both neurons and glia are killed, dead brain liquefies rapidly.
Liquefactive necrosis that is caused by neutrophilic leukocytes is calledpus.
Caseous necrosis • Caseousis derived from the gross appearance (pale yellow and cheesy) • All of the cells in an area die, • This is characteristic of a poorly-understood subtype of immune injury, and generally it is seen in certain granulomatous diseases: • Tuberculosis, • Fungal infections (coccidioidomycosis, blastomycosis, and histoplasmosis).