Download
1 / 25
270 likes | 807 Vues
FIBROUS DYSPLASIA: IMAGING CHARACTERISTICS. H . ZAGHOUANI BEN ALAYA, A.BEN ABDALLAH,S. YAHYAOUI, S. MAJDOUB,T. RZIGUA , L. BEN CHRIFA,H. AMARA, D. BEKIR, CH. KRAIEM Imaging department , Farhat Hached Hospital , Sousse, Tunisia. INTRODUCTION.

E N D
FIBROUS DYSPLASIA: IMAGING CHARACTERISTICS H. ZAGHOUANI BEN ALAYA, A.BEN ABDALLAH,S. YAHYAOUI, S. MAJDOUB,T. RZIGUA, L. BEN CHRIFA,H. AMARA, D. BEKIR, CH. KRAIEM Imaging department, FarhatHachedHospital, Sousse, Tunisia
INTRODUCTION • Fibrous Dysplasia (FD) of bone is a rare non-inheritable congenital disease. • It is characterized by a focal proliferation of fibrous tissue in the bone marrow leading to osteolytic lesions deformities and fractures. • FD can be presented in a monostoticor polyostotic form. • The complications are represented mainly by bone deformities and nerve compression
Introduction • The imaging appearance is often characteristic and allows in combination with the clinic findings the diagnosis • Authors attempted to highlight the interest of imaging in the diagnosis of FD. • The literature is reviewed to delineate radiologic features of monostotic and polyostotic fibrous dysplasia.
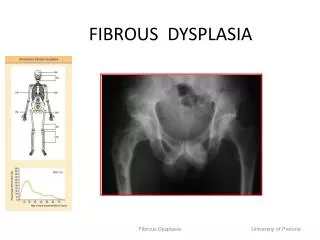
PATIENTS AND METHODS • Retrospective study of 7 cases. • FD was monostotic in 4 cases and polystotic in 3 cases • It involves proximal femurs in 1 case, ribs in 2 cases • 4 reported cases were craniofacial form and the involved bones were maxilla (n= 1), sphenoid (n = 1), temporal (n= 1), and frontal bone (n= 2) • Only 2 cases showed involvement of spine.
CASE N°1 • A 19-year-old boy presented to his doctor because of shoulder pain of 1 year’s duration. b (a) Well-defined lytic lesions of the humerus and both bones of the forearm, which at times appear multilocular and expansile with thinnes but unruptured cortical (b) CT showed in the medullary cavity replacement of cancellous bone with a homogeneous hyperdense beach responsible for thinning of the cortical a
Case n° 1 MR coronal images: *The lesions has low signal intensity on T1-weighted MR image (a ), highweightedintensity on T2 (b) *T1-weighted MR image with fat saturation and after administration of gadolinium (c ) show that there is mild to moderate heterogeneous enhancement of lesion. Polyostotic FD a b c *The same patient has cervical MRI for cervical pain that shows a lesion of the vertebral hemibody of D1 which has low intensity signal on T1 without cortical lysis or soft tissue abnormality on sagittal T1-weighted MR image (d). * T1-weighted MR image with fat saturation and after administration of gadolinium (e ) show that there is an intense enhancement of lesion. e d
CASE N°2 • A 24-year-old man whopresentswith a meningeal syndrome. A cerebro-medullar MRI wasindicated Monostotic FD of spine c *Sagittal T2-weighted MR image (a ) shows alow signal lesion of the vertebral body of D1 withan intense and homogene enhancement of the lesion on T1-weighted MR image (b ). *CT scan reveals increased bone density of D1 (c ). a b
CASE N°3 A 27-years-oldwoman , consultsfordiplopia lasting for 6 months. the clinicalexamination foundleft convergent squint and paralysis of the V and VI cranial nerves. a b c Coronal MR images show a lesion interesting the left greaterwing of sphenoid. This lesion has an intermediaire signal on T1 (a) , a low signal on T2 (b) and present an intense enhancement on contrast-enhanced T1-weighted MR image with fat-saturation (c ).
Case n° 3 Base of the skull (sphenoid) FD Axial and coronal CT scan show fibrous dysplasia involving body, the left greaterwing of sphenoid bone (blue arrows). Note expanded left pterygoid process (arrowhead) and inflammatory changes in left sphenoid sinus (*).
CASE N°4 A 35-yearoldwomanwhoconsulted for left frontal and orbital swelling Cranio-facial FD c a b *Axial T1-weighted MR (a ) and coronal T2-weighted MR (b) images reveal expansile lesion, with low signal intensity involving rleft frontal and parietal bones * Axial T1-weighted MR image with fat saturation and after administration of gadolinium (c ) show that there is mild to moderate heterogeneous enhancement of lesion.
CASEN°5 A 12-yearsold boy whopresented a ptosis of the left upper eyelid Cranio-facial FD a b c *Axial CT scan (a) show thickening and increasedfronto-orbital left bone density. *Coronal MR images show a lesion interesting left roof of orbit. This lesion has a low signal intensity on T1 (c) andT2 (b) . *T1-weighted MR image after administration of gadolinium (d ) show that there is intense and heterogeneous enhancement of the lesion. d
DISCUSSION • Fibrous dysplasia (FD) is a congenital and noninheritedbenignbonedisease • FD has been regarded as a developmental skeletal disorder characterized by replacement of normal bone with benign cellular fibrous connective tissue. • It affects both sexes with a slight female predominance and is diagnosed between 5 and 30 years on average
Discussion • It affects both sexes with a slight female predominance and is diagnosed between 5 and 30 years on average • The lesions grow with the child, stabilize afterpuberty and appearexceptionally in adulthood • FD can affect one bone (monostotic form) or multiple bones (polyostotic form), and the latter may form part of the McCune-Albright syndrome (MAS) or Mazabraud syndrome
MonostoticFibrousDysplasia • The monostotic form of FD comprises approximately 80% of all cases • It is seen in patients between 10 and 70yearsold. • The most common sites of involvement include the rib, femur, tibia, mandible, skull, and humerus • Solitaryinvolvement of other bones is unusual • FD of the spine is rare. It most commonly involves the body and adjacent pedicle without particularpredilection for a part of the spinal column
MonostoticFibrousDysplasia • The skull and facial bones are the affected sites in 10–25% • All bones of the skull and the face may be affected • It concerns mainly the ethmoid (72%), sphenoid (43%), the frontal bone (33%), maxilla (24%) and less frequently the temporal, parietal, occipital or mandible bone.
MonostoticFibrousDysplasia • Uncomplicatedmonostoticlesions are generallyasymptomatic and usually do not cause significantdeformity. • As a rule, monostoticfibrous dysplasia does not convert to the polyostoticform • lesions do not increase in size over time, and the disease becomes inactive atpuberty
PolyostoticFibrousDysplasia • The polyostotic form of FD may involve many or few bones, most commonly the skull and facial bones, pelvis, spine, and shoulder. • Polyostoticfibrousdysplasia is often unilateral, and may be bilateral, always asymmetric • It tends to involve larger segments of bone and is frequently associated with fractures and severe deformities.
PolyostoticFibrousDysplasia • Involvementof the skull may cause cranial nerve dysfunction with visual and hearing impairment • Although the manifestations of polyostotic fibrous dysplasia may be severe, it does not spread or proliferate and generally becomes quiescent at puberty, but existingdeformitiesmayprogress
Syndromes AssociatedwithFibrousDysplasia 1-McCune-Albright syndrome is an endocrinopathy occurring mainly in girls, consisting of the triad of precocious puberty, polyostotic FD, and characteristiccutaneous pigmentation referred to as “café au lait” spots 2-Mazabraud syndrome is the rare combination of fibrous dysplasia and soft-tissue myxomas
Imaging findings: radiograh and CT • Classically, fibrous dysplasia lesions are intramedullary, expansile, and well defined lesion with thick sclerotic borders • Althoughendostealscallopingmaybe present, a smooth cortical contour is always maintained • Lesions show varyingdegreesof hazy density with a ground-glass quality, although some may appear almost completelyradiolucent or sclerotic
Three types of lesions are distinguished depending on the degreeof hazy density : *The ground-glass pattern *The homogeneously dense pattern: increased bone density compared with adjacent normal bone *The cysticvariety: At times, a mubtilocubar, cystic lesion with well-defined marginscanbeseen • Occasionally, calcifiedcartilaginous and osseous foci may be presentwithin the lesion
MRI findings • The MRI characteristics of FD are variable • Typicallyshowing signal intensity that is intermediate to low on T1- weighted images • Intermediate to high signal on T2-weighted images • These high signal intensities on T2- weighted images correspond to nonmineralized areas and regions of cystic change • Fibrous dysplasia reveals varying degrees of enhancement after gadolinium infusion.
MRI findings • The fibrous tissues in FD are well vascularized and often show numerous small vessels in the center and large peripheral sinusoids. These histologic features explain why fibrous dysplasia enhances intensely after the injection of contrast material
Complications of FibrousDysplasia 1-Pathologic fracture • These fractures generally heal normally, but additional fractures may subsequently occur at the same site 2-Malignant degeneration of FD • Complicates less than 1% of all cases • Radiographicfindingsinclude cortical destruction and associated soft-tissue masses • The most common malignancies include osteosarcoma, fibrosarcoma, and malignantfibroushistiocytoma.
CONCLUSION • Fibrous dysplasia is a common benign bone disease existing in monostotic and polyostoticforms • Complications, and associations of fibrous dysplasia is important to ensure the accurate diagnosis and appropriate management of this disease • The imaging features of fibrous dysplasia are characteristic, althoughnot specific, and depend on the underlying histopathology of a given lesion.