Mycobacterium slowly growing
230 likes | 675 Vues
Mycobacterium slowly growing Mycobacterium tuberculosis , - Mycobacterium leprae, M.bovis, M.ulcerans Atypical mycobacteriaee – Runyon´s classification I.-IV. M.kansasi, M.marinum photochromatic

Mycobacterium slowly growing
E N D
Presentation Transcript
Mycobacterium • slowly growing • Mycobacterium tuberculosis , - Mycobacterium leprae, • M.bovis, M.ulcerans • Atypical mycobacteriaee – Runyon´s classification I.-IV. • M.kansasi, M.marinum photochromatic • M.scrofulaceum scotochromatic • M.avium, M.intracelulare sowly growing non pigmented • M.fortuitum, M.chelonae rapidly growing nonpigmented • Actinomycetes and nocardiae
Mycobacterium –genus non motile, non spores forming, aerobic rods Cell wall rich on lipids = hydrophobic surface = resistent to desinfectants = not stainable. If stained – heating – they resist decolorisation by strong acids = acideresistant, acid fast Slow growth M.tbc, M.leprae and from atypical . – group III of Runyon´s classification generation time 12-24 hrs – visible colonies after 3-8 weeks Group I., II. a IV. - 3 days and more M. leprae – non cultivated untill now 41 species - 27 isolated in human, 95% of which are M.tbc, M. avium-intracelulare, M.kansasii, M. foruitum, M. chelonae a M. leprae.
Cell wall – complex structure peptidoglycan(rigidity) + fosfodiesterically bound molecules of D- arabinose a D-galaktose on mycolic acid (most important lipid in the cell wall). + free lipids (wax, mycosides – cord factor) – responsible for paralel arrangement of bacilli in virulent strains + polypeptids (PPD) on the surface – antigenic, stimulation of cell immunity, extracted and purified is used in skin tests Polypeptid PPD Mycolic acid Arabinose, galktose with peptidoglycan Cytoplasma with plasmatic membrane
Growing factors and morphology of colonies – Speed of growth and pigmentation – classification sc. Runyon Slowly gorwig, nonpigmented – M. tbc...... I.group – photochomogenic– production of intense yellow carotenoid on the light II.group – scotochromogenic – production of pigment in dark and light III.group – slowly growing non pigmented IV.group – rapidly growing non pigmented
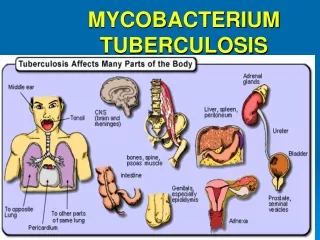
Pathogenesis and immunity Mycobacterium tuberculosis Destruction of tissue and fibrosis – answer of the host to the infection with M.tbc Intracelular parasit – escape the inborne immune mechanisme Tuberculosis – classic disease after inhalation of M.tbc * Engulfment by alveolar macrophages * Multiplication intracellularly –escape immune system destruction of fagocytes. * Repetition of this process (fagocytosis of bacilli, replication of M.tbc, lysis of cells = multilobular giant cells of macrophages„Langhans cells“ * Infected macrophages spread to local lymph nodes, blood vessels net, bone marrow,spleen, kidneys, bones, CNS...)
2-4 weeks after infection Cytokins produced by CD4 T lymfocytes activate macrophages,that are able to kill bacteria: low infectious dose – small tissue damage big infectious dose (masive infection) – large tissue damage (necrosis) Immune reaction: *cytokins produced by T lymfocytes, * activation of complement, * ischemia of the tissue * hydrolytical ensymes produced by macrophages Efficiency in eliminating of bacteriadepend on the extent and localisation of the infection: localised activated macrophages (granulome < 3mms): macrophages can penetrate in it and kill bacteria, stop spreading larger necroses, kaseous granulomas – surrounded by fibrin., bacteriae survive in the center, can be reactivated after years
Patogenesis and immunity ofMycobacterium leprae infection Lepra, Hansen´s disease Lepra lepromatosis – strong antibody respons, defect of cell immunity to M.leprae.Many bacteria in skin macrophages, very infectious forme Lepra tuberculoid – strong hypersensitive reaction (4th type), faible humoral antibody answer, many lymphocytes amd granulomes, few bacteriae in tissue (activated macrophages fagocytes bacteriae) Symptoms of the disease are produced by the immune answer of macroorganisme Other mycobacteriae:M.kansasí,M avium-intracellularegranulomatouse inflamation – localised lung infection, clinically identical as tbc., or disseminated. M.marinum, M.ulcerans: skin infection – prefer colder placesM.fortuitum, M.chelonae:very rare disseminated infection
Clinical signes M.tbc can involve any organ * lunga * extrapulmonal tbc * Tbc in HIV infected M.avium-intracellulare * lung ( in immunocompromised) * asymptomatic colonisation * disseminated disease in HIV positive M. leprae * Lepra lepromatosis, * Lepra tuberculoid Other mycobacteriosis * Lung (M.kansasií) * Skin (M. marinum,M.ulcerans)
Pulmonal tuberculosisafter inhalation of contaminated aerosol Inicial plung infection – multiplication 3-6 weeks, before the cell immunity is not activated 5% infected – active infection before 2 years after contact 5-10% later in life Nonspecific signs, little of sputum, rtg, positive skin test, laboratory verifiction by microscopy and cultivation. Active disease with pneumonia, abscess formation, cavities with big involvement of lobes. Extrapulmonal tbc – hematogenous dissemination during inicial phase (lymphnodes, pleura, UGT) – not necessary signs of lung involvement Tbc in HIV positivity – decreasing part of CD4 lymfocytes, infection is before other of oportunistic infections
Laboratory diagnosisMicroscopy rapid dg, Ziehl Neelsen, fluorescence, preparation of the sample, Cultivation morning sputum 3 consecutive days or a big ammount of other liquid – urine, * slow growth * overgrowth of contaminating bacteria - *decontamination + NaOH, * egg media Genetic probes detection of Am.Acid sequention, 6 hrs. Directly from material Serologynot sensitive, nor specific Detection of activation of specific lymfocytes – interferon production
Clinical diagnosis and therapy: Skin testi.d 0,1 mcg = 5TU application PPD purified protein derivate od cell wall 48 later <15mm negat – without reaction, anergia ( HIV infected olso), 15 mm OK >15mm – contact with M.tbc in surroundings, or disease Resistenceon common, longlasting therapy (18 –24 mnths 6-9 mnths), rapid development of resistence = combination of INH, rifampicin, pyrazinamid, ethanbutol,streptomycin + cycloserin(atypical), chinolons(for other infection) 1990 multiresistence USA in HIV patients Rapidly growing mycobacteria – very resistent M.leprae rapid resistence – combination of dapson+rifampicin, clofazimin+etionamid
Prevention Chemoprophylaxis INH 1 year in case of contact with M.tbc or positivity in skin test - hepatotoxicity Vaccination attenuated strain M. bovis - bacillus Calmette Guerin–BCG – living strain 5th day after birth, reactions – BCG-itis – positivity of skin test ! a interpretation
Epidemiology – trasmission of the infection M.tbc Persons are the only reservoir Transmission via a close longlasting contact with the ill person – inhalation Particules of aerosol with 1-3 tbc bacili can reach lung alveoli 5-200 bakteria can cause the infection Homeless, alcoholics, drug abusers, HIV patients ATB resistance
Epidemiology – trasmission of the infection Other mycobacteriae M. bovis – infection of annimals, source for human infection - milk M.avium-intraellulare complex – present in water and soil, annimals and birds. Transmission via food in immunocompromised and HIV infected M.leprae12 milions, 62% in Asia, 34% v Africa, transimission by long contact with the infected person, inhalation, skin contact with secreted fluids from nose, exudations from wounds or by insect vector
Antituberculotics and therapy • Streptomycin(kill actively multiplying M.tbc) Izoniazid,Rifampicin (effective on M.tbc in caseous necrosis) Ethanbutol Etionamid Kanamycin Cycloserin Pyrazinamid ( active i.c.) • In pacient with pulmonar tbc - 3 populations of M.tbc - localised extracelullarly in cavitas, - intracelullarly in macrophages, - inside caseouse necrosis • Combination of 2-3 ATT. Resistence fighting -overgrowinf of resistent mutants in culture of M.tbc - for INH 1:105 for STM 1:106 in infectious place there is 107- 10 9 of bacteria
ATB susceptibility • Susceptibility test for antituberculotics - ATT are dissolved in medium • Method of proportional susceptibility testing - dilution method. Dilution of inoculum so that there is from 100-300 CFU - colony forming units on a plate • If there is more than 1% of M. tbc cells resistent to ATT the therapy will not be cliniccňally suscessful
Spontaneous appearance of resistent mycobacteria - without exposition to ATT • Frequency of resistent cells in the culture is 1:105 for INH and 1:106 for STM - if both are given in combination the incidence of resistent strains will be 1:1011. • The overall population of bacilli in patient with open cavity is 10 7 - 109 , so there is 102 - 104 resistent strains. • 1 ATT means overgrowing of resistent strains that will replace susceptible killed bacteria. • Combination of 2 and more ATT: INH+RIF - 9 months, + STR+ Ethanbutol for 2-8 weaks, from 2nd months only 2 times weakly, INH + Ethanbutol 18-24 months,
Tests for ATT susceptibility - correlation between in vitro and therapy success. • If more than 1% of M. tbc in vitro are resistent - therapy will not be successful • Tests determine ratio between susceptible and resistent strains • Agar dilution method - depend on innoculum - if too thick - there is too much of resistent strains - false resistent, if less concentrated - false positive - possible resistent strains not identified. • Optimal dilution 100-300 CFU on plate • Inconvenience - aga can inhibit activity of ATT as well as of mycobacteria, long incubation decrease activity of ATT
Principles of therapy • Therapy: ATT are active only on growing mycobacteria, growth depends on oxygen availability and pH (optimu neutral or alkaline) - Max in open cavity, min in caseouse necrose. • In i.c. - in phagosomes - pH is 5,5, acid - slow growth, less of bacilli, less resistent strains - ATT supporting acid environment - Pyrazinamide. (STM not able to enter phagosomes and looses activity in acid pH) • in chronic closed caseouse necrose - slow blood supply and oxygen, slow metabolism, less living cells, pH neutral but slow multiplication
ATT • Bactericidal: STM - mycobacteria extracellularly in cavities • INH - kills slowly and quickly growing cells • Rifampicin - effective on mycobacteria closed in caseouse necrosis and macrophages • Pyrazinamide - only in acid pH and in macrophages • Bacteristatic: Ethanbutol - only in combination, able to penetrate in mycobacteria situated i.c. and e.c. • Capreomycin, Kanamycin - bactericidal, for e.c mycobacteria in cavities • Ethionamid, cycloserin - bacteriostatic for i.c and e.c